

Perfect B, Doral Fl. | 05.06.26 | 9 min read.
This post is for educational purposes only and does not constitute medical advice. Peptides are prescription compounds in many contexts. Consult a licensed provider before beginning any peptide or NAD+ protocol.
What Biohacking Peptides Actually Means in a Clinical Setting
Online, biohacking peptides has become a catch-all phrase that bundles unregulated injections, gym-bro stacks, and direct-to-consumer compounds into one category. In a clinical setting at Perfect B in Doral, FL, biohacking peptides means something narrower and more useful. It refers to the structured use of peptide therapy, supported by baseline labs and a sequenced protocol, to influence specific biological pathways your body is no longer running efficiently.
Peptides are short chains of amino acids that act as biological messengers. They tell cells to repair, signal hormones to release, regulate inflammation, or support recovery. The clinical question is not whether peptides do something. They do. The question is whether you actually need a given peptide, at what dose, for how long, and under what monitoring. That is the gap between marketing and medicine, and it is where Perfect B operates.
Key Takeaways
- Biohacking peptides only works when paired with baseline testing, not when chosen from a popular stack list or purchased through unregulated channels.
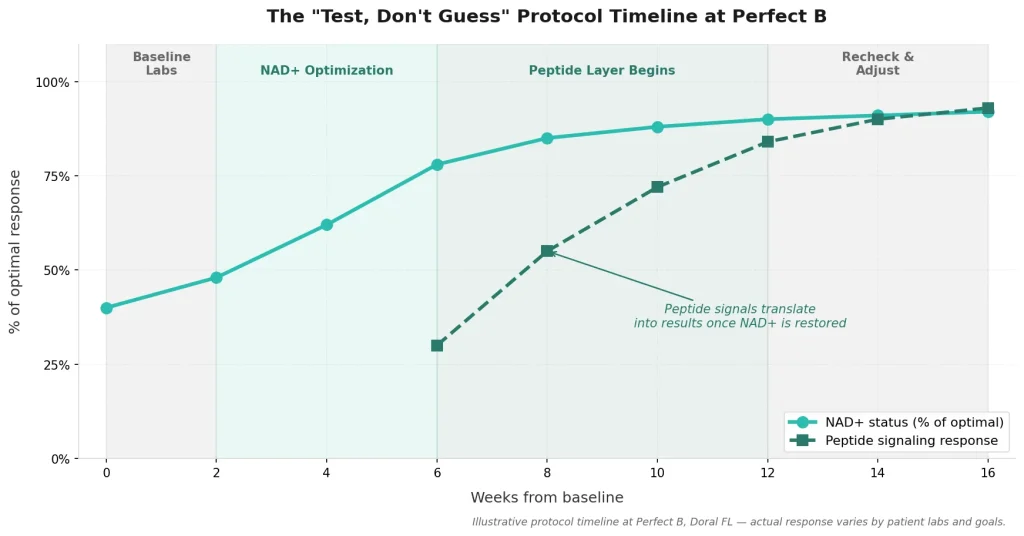
- NAD+ optimization comes before peptide therapy at Perfect B, because peptide signals fail to translate into results when cellular energy is depleted.
- The “Test, Don’t Guess” protocol replaces guesswork with measurable inputs, including intracellular NAD+, hormone panels, and inflammation markers.
- Compounding quality and supervision are non-negotiable, especially given recent FDA and NPR coverage of peptide safety concerns in unregulated markets.
- Women require a different peptide calibration, with attention to cycle phase, iron status, and estrogen timing rather than a male-default protocol.
The “Test, Don’t Guess” Protocol: Why Baseline Labs Come Before Any Peptide
Most peptide failures we see at Perfect B are not failures of the peptide itself. They are failures of context. A patient with low ferritin, suboptimal thyroid function, or chronically poor sleep will not respond to a recovery peptide the way the marketing suggests, because the underlying biological environment cannot translate the signal into results.
Our protocol begins with baseline data. For most patients considering peptide therapy, we run a metabolic panel, thyroid function, ferritin, vitamin D, and intracellular NAD+ when clinically indicated. For specific goals, we add hormone panels or inflammation markers. The labs tell us whether peptides are the right next step, whether we need to address something more fundamental first, or whether the patient does not actually need peptides at all.
This sounds slow compared to a clinic that prescribes peptides on the first visit. It is. It is also the reason patients at Perfect B see consistent results rather than the wide variability that defines unsupervised peptide use. We test, we read the data with the patient, and we design a sequenced plan rather than a default stack.
NAD+ as the Foundation: Why It Comes Before Peptides at Perfect B
Nicotinamide adenine dinucleotide, or NAD+, is the coenzyme your cells use to convert food into usable energy, repair DNA, and regulate the SIRT1 and AMPK pathways that govern training adaptation and recovery. NAD+ levels decline measurably with age, becoming suboptimal in many patients after 35 and dropping significantly in the decade between 40 and 60.
Here is why this matters for peptide therapy: peptides are signals. Cells with adequate NAD+ can act on those signals. Cells running on depleted NAD+ cannot, or do so inefficiently. A growth-related peptide given to a patient with severely low NAD+ will produce muted results that the patient often interprets as the peptide not working. The peptide was working. The infrastructure to act on it was not in place.
At Perfect B we test intracellular NAD+ before recommending NAD+ supplementation, and we prefer non-IV approaches for most patients because they support steadier baseline restoration without the rebound effects some patients experience after IV-only protocols. When NAD+ is optimized first, peptide protocols layered on top of it tend to produce the response patients expected from the peptide alone.

Peptides That Work With Optimized NAD+: Categories, Not Stacks
The peptide world is overwhelming when you encounter it through forums and influencer content. Inside our clinic, we organize peptides by what they do, not by what is trending. The categories below are the ones we discuss most often with patients during a peptide consult.
Recovery and Tissue Repair Peptides
These peptides influence the body’s repair signaling. They are the category most relevant to athletes, post-procedure patients, and individuals dealing with chronic soft tissue irritation. Used inside a supervised protocol, with baseline labs and dosing aligned to body weight and goal, they produce measurable improvements in recovery time and inflammatory markers.
Growth Hormone Releasing Peptides
This category includes peptides that prompt your pituitary to release more of your own growth hormone in a pulsatile pattern, which is closer to natural physiology than direct hormone replacement. We screen patients carefully before considering these, and we monitor labs through the protocol. Not every patient who asks for a GH-related peptide is a candidate for one.
Skin and Aesthetic Peptides
Distinct from systemic peptides, these are typically applied topically or used in conjunction with aesthetic procedures. They support collagen quality, pigmentation, and recovery from energy-based treatments. We treat them as a separate category from systemic peptide therapy because the clinical considerations differ.
What we do not do at Perfect B is hand patients a stack pulled from a forum. The combination, the dosing, the duration, and the monitoring are designed for your labs and your goals, not for a generic protocol someone published on Reddit.

Safety, Compounding Quality, and What Recent Coverage Often Misses
Recent media coverage, including reporting from NPR, has highlighted safety concerns around peptide use. The concerns are real, and they almost always center on the same two issues: unregulated source quality, and use without medical supervision. Both of those issues disappear when peptides are prescribed by a licensed clinician and dispensed through a reputable compounding pharmacy with documented quality controls.
At Perfect B, peptides are prescribed when they are clinically appropriate, sourced through compounding pharmacies that we vet for purity and consistency, and monitored through follow-up labs and clinical check-ins. We do not sell peptides as wellness products. We prescribe them as part of a medical protocol or we tell the patient that peptides are not the right fit for their situation.
Patients who proceed with caution or modified protocols include those with active cancer diagnoses, certain autoimmune conditions, pregnant or nursing women, and individuals with significant liver dysfunction. Some peptides are specifically contraindicated in oncology contexts, and our screening reflects that. The conversation about peptides should always start with whether they are safe for you, not with which one to order.
Biohacking Peptides for Women: A Different Calibration, Not a Smaller Dose
Female peptide protocols are not male protocols at lower doses. They require a different framework. The menstrual cycle changes how women respond to recovery, training load, and certain hormone-related signals. Iron status, often overlooked in female patients, can blunt the response to recovery peptides regardless of dose. Thyroid function and estrogen status interact with several peptide categories in ways that male-default protocols simply do not address.
For women in perimenopause and menopause, the considerations shift again. Estrogen decline reshapes recovery, sleep architecture, and body composition in ways that influence which peptides are clinically useful and at what timing. We design protocols around those realities rather than ignoring them. That is the calibration that distinguishes clinical biohacking from a male-default stack repackaged for a female patient.
Frequently Asked Questions
1. Do I need NAD+ testing before starting peptide therapy?
For most adults over 35 considering peptide therapy at Perfect B, yes. Intracellular NAD+ testing tells us whether the cellular energy environment can support what the peptide is trying to do. If NAD+ is significantly depleted, we usually address that first or in parallel, because peptide signals work better when cells have the energy to act on them.
2. How is this different from buying peptides online?
The differences are quality, supervision, and personalization. Peptides bought online have variable purity, no dosing customized to your labs, and no clinician monitoring outcomes. At Perfect B, peptides are prescribed when clinically indicated, sourced from compounding pharmacies we vet, and adjusted based on follow-up labs and your response. The price difference reflects the medical work behind the prescription, not just the compound.
3. Why does Perfect B prefer non-IV NAD+ approaches?
Non-IV approaches support steadier baseline NAD+ restoration with less of the rebound variation some patients experience after IV-only protocols. IV NAD+ has its place in specific clinical scenarios, but for most patients pursuing biohacking peptides alongside NAD+ optimization, non-IV options produce more consistent intracellular results over time. The decision is always made based on labs and clinical context.
4. Are peptides safe long-term?
Safety depends on the specific peptide, the dose, the duration, the source, and the patient. Peptides that are appropriate for a healthy adult after baseline screening, sourced through a vetted compounding pharmacy, and monitored through follow-up labs have a strong safety record in clinical use. Peptides bought from unregulated sources and used without monitoring have a very different risk profile. The category is not inherently safe or unsafe. The protocol determines the answer.
5. How long before I see results from a peptide protocol?
Recovery and inflammation-focused peptides often produce noticeable changes within two to four weeks. Growth hormone releasing peptides typically require eight to twelve weeks of consistent protocol use before the cumulative effect on energy, recovery, and body composition becomes apparent. Skin and aesthetic peptides follow the timeline of the procedure they accompany. We set expectations based on the peptide and your baseline labs at the start of every protocol.
6. Can I combine peptides with other treatments at Perfect B?
Often yes, and sequencing is part of the design. Peptides combine well with NAD+ optimization, supervised nutrition coaching, and most aesthetic procedures with appropriate spacing. Some combinations require timing adjustments to avoid interfering with tissue repair or recovery windows. Your provider will outline what to combine, what to space out, and why during your consultation.
Closing: The Clinical Bottom Line on Biohacking Peptides
Biohacking peptides is not a shortcut. It is a structured clinical process that pairs the right peptide with the right patient at the right point in their plan. The work that distinguishes Perfect B from a forum-driven stack is the work most patients never see: the labs we run, the conversations we have about whether a peptide is even the right step, and the follow-up that adjusts the plan as your data evolves.
If you have been considering peptides, the most useful next step is rarely to choose a peptide. It is to find out what your labs say. From there, the protocol becomes specific, measurable, and yours.
📍 Visit us at Perfect B, Doral FL
📞 Call or message us at (786) 502-2260


