

Valeria Marulanda is a board-certified Family Nurse Practitioner (FNP-BC, NPI 1841152584) specializing in medical aesthetics at Perfect B in Doral, FL.
Are peptides and Ozempic the same thing?
Yes and no. Ozempic (semaglutide) is technically a peptide, but “peptide therapy” usually refers to a different class of peptides that activate your body’s own pathways rather than mimicking a single gut hormone. At Perfect B in Doral, FL, we use three peptides for weight and metabolic goals: tesamorelin (FDA-approved for visceral fat), MOTS-c (mitochondrial metabolism), and CJC-1295/Ipamorelin (growth hormone optimization).
Perfect B, Doral Fl. | 05.13.26 | 11 min read.
This content is for educational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before starting any peptide or weight loss therapy.
Key Takeaways: 5 Things to Know Before Comparing Peptides and Ozempic
- Ozempic is itself a peptide, specifically a synthetic GLP-1 receptor agonist, but the term peptides for weight loss covers a much broader category of molecules with different mechanisms.
- Non-GLP-1 peptides like AOD 9604, Tesamorelin, and CJC-1295/Ipamorelin target fat metabolism and growth hormone rather than appetite suppression.
- Ozempic and similar GLP-1 drugs produce rapid weight loss but come with well-documented trade-offs: nausea in up to 40% of patients and significant muscle mass reduction.
- Non-GLP-1 peptides work more gradually but preserve and in many cases improve lean muscle mass, making them a different tool with a different ideal patient.
- The right choice depends on your metabolic profile, body composition goals, and tolerance for side effects. Lab work before any protocol is non-negotiable.
Is Ozempic Actually a Peptide? Why the Answer Changes Everything
Yes. Ozempic (semaglutide) is a synthetic glucagon-like peptide-1 receptor agonist. It is a peptide in the strict biochemical sense: a chain of amino acids designed to mimic and amplify the action of GLP-1, a hormone the gut naturally releases after eating.
But when most people search for peptides for weight loss, they are not looking for semaglutide. They already know what Ozempic is. What they want to understand is whether there are other peptide-based options, what those options do, and how they compare to what is now the dominant name in injectable weight loss.
That distinction matters because it changes the entire conversation. GLP-1 drugs like Ozempic work by suppressing appetite and slowing gastric emptying, and a 2025 Stanford Medicine study identified a naturally occurring peptide that rivals semaglutide for weight loss while avoiding nausea and muscle loss. The peptides used in regenerative medicine clinics across South Florida work through entirely different pathways, targeting fat metabolism, growth hormone secretion, and cellular energy directly. Understanding that difference is the starting point for making an informed decision.

How GLP-1 Drugs Like Ozempic Work and the Trade-offs Patients Should Know
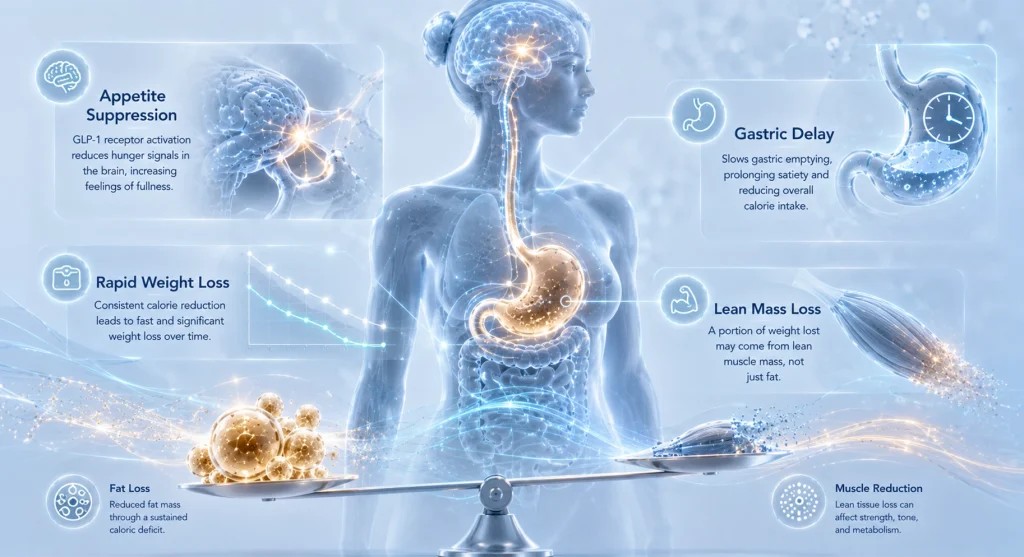
The mechanism: appetite suppression and gastric delay
GLP-1 receptor agonists work primarily by binding to receptors in the brain and gut that regulate hunger. They slow the rate at which food leaves the stomach, reduce appetite signals, and improve insulin sensitivity. The result is that patients eat less, feel full faster, and lose weight at a rate that exceeds most other pharmacological interventions.
A 2025 Stanford Medicine study identifying a naturally occurring peptide that suppressed appetite and reduced body weight without the nausea and muscle loss associated with semaglutide confirmed what many clinicians had already observed: the GLP-1 mechanism is powerful, but it carries side effects tied directly to how it works.
The trade-offs that matter clinically
- Nausea and GI symptoms: Reported in 30 to 44% of patients on semaglutide. For many, this is transient. For others, it limits dosing or leads to discontinuation.
- Muscle mass loss: Multiple studies confirm that a significant portion of weight lost on GLP-1 drugs is lean muscle, not fat. This is the mechanism behind what has been called “Ozempic face” and similar body composition changes.
- Rebound on discontinuation: Most patients regain a substantial portion of lost weight within 12 months of stopping treatment, because the underlying metabolic drivers were not addressed.
- Cost and access: Branded semaglutide remains expensive and subject to supply shortages, pushing patients to explore semaglutide alternatives.
None of this means GLP-1 drugs are the wrong choice. For patients with clinical obesity, type 2 diabetes, or cardiovascular risk that requires rapid medical intervention, they remain one of the most effective tools available. The question is whether every patient searching for peptides for weight loss has that profile. Most do not.
The Other Category: Non-GLP-1 Peptides That Target Fat Through a Different Mechanism
The peptides used at regenerative medicine clinics for fat loss are not the same as Ozempic. They do not suppress appetite. They do not slow your digestion. They work at the cellular level, interacting with fat cells, growth hormone receptors, and metabolic pathways directly.
Two completely different approaches
- GLP-1 drugs (Ozempic, Wegovy, Mounjaro): Reduce food intake and slow digestion. Weight comes off because you are eating less. The risk: muscle follows fat downward.
- Non-GLP-1 metabolic peptides (AOD 9604, Tesamorelin, CJC-1295/Ipamorelin): Act on lipolysis, growth hormone release, and metabolic rate. The body breaks down stored fat more efficiently, independently of what you eat.
This is why the comparison between peptides vs ozempic is not as simple as asking which one causes more weight loss. They are answering different questions for different patients. A patient who needs to lose 60 pounds for medical reasons may belong on a GLP-1. A patient who is already metabolically healthy and wants to reduce visceral fat while preserving muscle may get far more value from a non-GLP-1 protocol.
Not sure which peptide protocol fits your goals?
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.

AOD 9604: The Fat-Burning Peptide That Acts Directly on Adipose Tissue
What AOD 9604 actually is
AOD 9604 is a synthetic fragment of human growth hormone, specifically the C-terminal region (amino acids 176 to 191) responsible for stimulating fat breakdown. It was originally developed as a safer alternative to hGH for metabolic applications, and it is now one of the most used peptides for weight loss in supervised clinical settings. For a detailed clinical overview, see our published guide on AOD 9604 and how this HGH fragment targets visceral fat without suppressing appetite.
How it works at the cellular level
Unlike semaglutide, AOD 9604 does not interact with appetite centers. It binds directly to fat cells and stimulates lipolysis, the process by which stored triglycerides are broken down into free fatty acids the body can burn. Critically, it does this without activating the insulin-like growth factor pathway, which means no blood sugar disruption and no proliferative risk.
What patients notice and when
- Weeks 1 to 4: Subtle changes in energy and early shifts in how clothes fit, particularly around the midsection.
- Weeks 5 to 12: Measurable reduction in subcutaneous fat, especially in stubborn areas like lower abdomen and flanks.
- Weeks 12 to 20: Most patients see their clearest results during this window, with consistent protocol adherence.
- Best results: AOD 9604 works best when combined with adequate protein intake and a resistance training program, which preserves the lean mass the GLP-1 drugs tend to erode.
For the patient who asks why they should consider AOD 9604 rather than just going on Ozempic, the honest answer is candidate profile. AOD 9604 is the right peptide for someone who is already metabolically functional, who wants to address specific fat compartments, and who cannot tolerate or is not a clinical candidate for GLP-1 therapy. Read more in our detailed guide on AOD 9604 and how this HGH fragment works to reduce visceral fat without suppressing appetite.
Tesamorelin and Visceral Belly Fat: What the Clinical Data Shows
The FDA approval that makes Tesamorelin different
Tesamorelin is the only non-GLP-1 peptide in this category with an FDA approval for body fat reduction. It is approved specifically for visceral adiposity associated with HIV-related lipodystrophy, but the clinical data on its mechanism extends beyond that narrow indication. As a growth hormone-releasing factor (GRF) analogue, Tesamorelin stimulates the pituitary gland to release natural growth hormone in a pulsatile, physiological pattern. A peer-reviewed review in Frontiers in Endocrinology summarizing peptide mechanisms and clinical potential for obesity and metabolic dysregulation provides the scientific framework behind this class of treatments. For our clinical overview of how this works in practice, see our complete guide to Tesamorelin and its documented effect on abdominal fat reduction in South Florida patients.
What the clinical data shows on belly fat
Controlled trials have demonstrated reductions of 15 to 20% in visceral adipose tissue over 26 weeks of treatment. Visceral fat, the kind stored around organs in the abdominal cavity rather than under the skin, is directly linked to metabolic syndrome, insulin resistance, and cardiovascular risk. This is the fat that GLP-1 drugs do reduce, but Tesamorelin targets it through growth hormone pathways rather than appetite suppression.
A peer-reviewed review in Frontiers in Endocrinology summarizing the mechanisms and clinical potential of peptide-based interventions for obesity and metabolic dysregulation provides the scientific foundation that positions Tesamorelin and similar peptides as credible tools in weight management beyond the GLP-1 paradigm.
The key difference from Ozempic: muscle preservation
- Ozempic and muscle: A meaningful portion of weight lost on semaglutide is lean mass. Some studies report muscle loss accounting for 25 to 40% of total weight reduction.
- Tesamorelin and muscle: Growth hormone protocols consistently show preservation of lean body mass alongside fat reduction. Some patients see modest improvements in muscle density during treatment.
- Lipid profile: Tesamorelin has also been shown to improve triglyceride and HDL ratios, adding a cardiovascular benefit separate from fat loss.
The cycling protocol matters here. Tesamorelin is typically run in 3-month active cycles with a 2-month rest period. This prevents receptor desensitization and mirrors the way the body naturally regulates growth hormone. Learn more about our clinical overview of Tesamorelin and its documented effect on abdominal fat reduction in South Florida patients.
Not sure which peptide protocol fits your goals?
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
CJC-1295 and Ipamorelin: Body Composition Through Growth Hormone Optimization
How the stack works
CJC-1295 is a growth hormone-releasing hormone analogue with DAC (drug affinity complex), which extends its half-life and allows stable, sustained GH elevation. Ipamorelin is a selective ghrelin receptor agonist that stimulates a clean, pulsatile GH release without the cortisol and appetite spikes associated with older secretagogues like GHRP-6. For a full breakdown of how this combination works, see our explanation of how CJC-1295 and Ipamorelin work together to optimize growth hormone and improve body composition.
Combined, CJC-1295 and Ipamorelin produce a synergistic growth hormone pulse that the body recognizes as physiological, which minimizes feedback suppression and side effects. The result is a sustained elevation of IGF-1 and free fatty acid mobilization over several months of use.
Body composition versus weight loss: why this distinction matters
CJC-1295/Ipamorelin does not produce the dramatic scale changes that GLP-1 drugs do in the first 12 weeks. What it produces is a shift in body composition: less fat, more lean tissue, better metabolic function. For patients who measure success by how they look and perform rather than by a number on a scale, this is often a more satisfying outcome.
- Months 1 to 2: Improved sleep quality, faster recovery, subtle shifts in energy. Fat loss not yet visible on the scale.
- Months 3 to 4: Measurable reduction in body fat percentage, particularly subcutaneous fat. Lean mass holding steady or improving.
- Months 5 to 6: Most patients report the clearest visual changes in this window, with improvements in abdominal definition and overall leanness.
This timeline is longer than Ozempic. But the results tend to be more durable because the underlying metabolic drivers have changed, not just suppressed. Read our full protocol guide in our explanation of how CJC-1295 and Ipamorelin work together to optimize growth hormone and improve body composition.
Peptides vs Ozempic Side by Side: Mechanism, Timeline, Muscle Impact, and Cost
No comparison chart tells the whole story, but this one gives you the framework for the conversation you should have with your provider:
| Criteria | Ozempic (Semaglutide) | AOD 9604 | Tesamorelin | CJC-1295 / Ipamorelin |
|---|---|---|---|---|
| Primary mechanism | GLP-1 receptor agonist, appetite suppression | Direct lipolysis in adipocytes | GH-releasing factor, visceral fat reduction | GH secretagogue stack, body recomposition |
| Speed of fat loss | Fast (weeks 4 to 12) | Moderate (weeks 8 to 16) | Moderate (weeks 8 to 20) | Gradual (months 3 to 6) |
| Muscle mass impact | Significant loss (25 to 40% of weight lost) | Preserved or improved | Preserved, sometimes improved | Preserved and improved |
| GI side effects | Common (nausea 30 to 44%) | Minimal | Minimal | Minimal |
| FDA status | Approved for weight loss (Wegovy) | Not FDA-approved for weight loss | FDA-approved for visceral adiposity | Not FDA-approved for weight loss |
| Est. monthly cost (clinic) | $500 to $1,200+ branded | $200 to $400 compounded | $300 to $600 compounded | $150 to $350 compounded |
| Best candidate | Clinical obesity, diabetes, rapid intervention | Stubborn fat, active patient, no GI tolerance | Apple-body shape, visceral fat priority, muscle preservation | Body recomposition, active adults, long-term |
This comparison between peptides vs ozempic reflects general clinical patterns, not individual predictions. Your response to any protocol depends on your baseline metabolic health, current body composition, and how consistently you execute the protocol.
Who Should Choose Ozempic-Type Peptides vs. Non-GLP-1 Peptides?
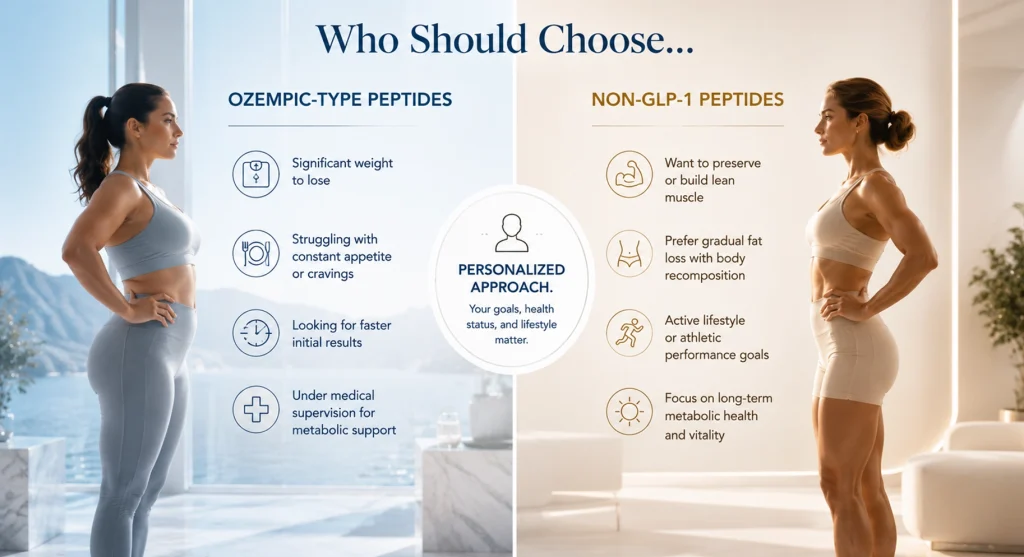
The patient profile for GLP-1 drugs
- BMI over 30 with metabolic complications: Type 2 diabetes, prediabetes, or significant cardiovascular risk factors.
- Rapid clinical intervention required: A patient whose health timeline demands fast, measurable results under medical supervision.
- No contraindications to GI side effects: Patient can manage or tolerate nausea during the titration period.
- Muscle loss acceptable: Patient prioritizes scale weight over body composition ratio.
The patient profile for non-GLP-1 peptides
- Metabolically healthy baseline: Fasting glucose, insulin, and lipids are within range, but stubborn fat remains.
- Body recomposition as the goal: Patient wants less fat and more lean mass, not just a lower number on the scale.
- Active lifestyle: Patient exercises regularly and does not want to compromise muscle during a fat loss phase.
- GLP-1 intolerance or non-candidacy: Patient has tried GLP-1 therapy and could not tolerate it, or is not a clinical candidate.
- Long-term sustainable change: Patient is willing to invest 3 to 6 months for durable metabolic improvement.
When both can be considered together
In some cases, a combination protocol is appropriate. A patient may use a low-dose GLP-1 to manage appetite while running AOD 9604 or Tesamorelin to specifically target visceral fat and preserve muscle. This requires careful medical supervision and regular bloodwork to monitor metabolic markers. It is not a DIY protocol.
Not sure which peptide protocol fits your goals?
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
What to Expect from Peptide Therapy for Fat Loss at a Medical Clinic in Doral, Miami
At Perfect B in Doral, FL, no peptide protocol starts without a full assessment. The weight loss injection landscape has too many providers offering one-size-fits-all protocols based on a brief online intake form. The patients who see the most consistent results are the ones whose protocols were built around actual data.
Step 1: Consultation and body composition assessment
Your first appointment covers your health history, current medications, fat loss goals, and lifestyle factors. We review any prior experience with weight loss peptides or GLP-1 drugs, including what worked and what did not.
Step 2: Lab work
Before recommending any protocol, we require a baseline metabolic panel that includes fasting insulin, IGF-1, fasting glucose, a lipid panel, and body fat percentage. These numbers determine which peptide or combination of peptides is appropriate for your specific situation.
Step 3: Protocol selection and initiation
Based on your labs and goals, we design a protocol. A patient with elevated visceral fat and good metabolic markers may start on Tesamorelin. A patient looking for body recomposition with muscle preservation may begin a CJC-1295/Ipamorelin stack. A patient with stubborn subcutaneous fat may benefit most from AOD 9604. Some patients run a combination. The protocol is specific to you, not to a category.
Step 4: Follow-up cadence
Check-ins at weeks 4, 8, and 12 allow for dose adjustments based on how your body is responding. At the 3-month mark, labs are repeated to track metabolic changes and confirm the protocol is delivering the expected tissue-level response. Weight loss injections in the Miami area are available at clinics ranging from weight loss chains to medical spas. The difference at a clinic like Perfect B is the data behind every decision.
To schedule a consultation, call us at (786) 502-2260.
Frequently Asked Questions
1. Do peptides for weight loss really work?
Yes, but the answer depends on which peptides you are asking about and what you define as working. GLP-1 receptor agonists like semaglutide produce 15 to 20% body weight reduction in clinical trials. Non-GLP-1 peptides like Tesamorelin have demonstrated 15 to 20% reduction in visceral fat in controlled studies. AOD 9604 and CJC-1295/Ipamorelin produce body composition changes that are measurable but more gradual. All of them work. None of them replaces a functional metabolic foundation.
2. What is the best peptide for weight loss?
There is no universal answer. The best peptide for weight loss is the one that matches your metabolic profile, your goals, and your tolerance for side effects. If rapid scale-based weight loss under medical supervision for a serious metabolic condition is the goal, a GLP-1 may be appropriate. If body recomposition, visceral fat reduction, and muscle preservation are the priorities, a non-GLP-1 protocol is likely a better fit. Lab work and a clinical consultation determine which path is right for you.
3. Is Ozempic a peptide?
Yes. Ozempic (semaglutide) is a synthetic GLP-1 receptor agonist, which makes it technically a peptide. However, when people search for peptides vs ozempic, they are usually asking about non-GLP-1 peptides used in regenerative and aesthetic medicine, such as AOD 9604, Tesamorelin, and CJC-1295/Ipamorelin. These operate through completely different mechanisms.
4. What are the negatives of taking peptides for weight loss?
The negatives depend on the peptide. GLP-1 drugs carry the most widely reported side effects: nausea, vomiting, constipation, and muscle loss. Non-GLP-1 peptides like AOD 9604 and Tesamorelin have a much cleaner side effect profile in clinical use, with injection site reactions being the most common issue. The broader risk with any peptide therapy is using unregulated, online-sourced peptides without medical supervision. This is where the majority of reported adverse outcomes originate.
5. How long do weight loss peptides take to work?
GLP-1 drugs produce visible results in 4 to 8 weeks for most patients. Non-GLP-1 peptides typically show measurable changes at 8 to 12 weeks, with the clearest results at 16 to 24 weeks. CJC-1295/Ipamorelin is the slowest of the group, with optimal body composition results at months 4 to 6. The tradeoff for the longer timeline is better durability and muscle preservation.
6. Can you use peptides and Ozempic at the same time?
In some supervised clinical contexts, yes. A provider may combine a low-dose GLP-1 for appetite regulation with a non-GLP-1 peptide for targeted fat metabolism and muscle preservation. This is not a protocol to pursue without a qualified physician managing both sides of the equation. The interaction between appetite suppression and growth hormone secretion requires careful monitoring.
7. Do you need a prescription for weight loss peptides?
GLP-1 drugs like Ozempic and Wegovy require a prescription and are tightly regulated. Non-GLP-1 peptides like Tesamorelin, AOD 9604, and CJC-1295/Ipamorelin are available through licensed compounding pharmacies and require a prescription from a licensed provider. Any clinic offering these peptides without a medical intake, consultation, and prescription process is not operating within safe clinical standards.
Closing: The Clinical Bottom Line on Peptides vs Ozempic in South Florida
The debate between peptides and Ozempic is often framed as a binary. It is not. GLP-1 drugs and non-GLP-1 peptides are different tools built for different patients with different goals. The patient who needs rapid, clinically significant weight loss for diabetes management is not the same patient as the one who wants to reduce visceral fat while preserving the lean mass they have built over years of training. Treating them the same way produces worse outcomes for both.
At Perfect B in Doral, FL, the approach is to let your lab work and your goals determine the protocol, not a trend or a one-size-fits-all menu. If you are somewhere in South Florida researching peptides for weight loss and trying to figure out whether your profile fits a GLP-1 pathway or a non-GLP-1 peptide protocol, that conversation starts with a consultation and a metabolic panel, not a quiz or a package price.
📍 Perfect B | 8200 NW 41st St, Suite 100, Doral, FL 33166
📞 (786) 502-2260
→ Explore our Peptide Treatment Plan at Perfect B in Doral, FL and see which protocol fits your goals.


