

Perfect B, Doral Fl. | 05.21.26 | 12 min read.
This article is for educational purposes only and does not substitute professional medical advice. Always consult a licensed medical provider before starting any peptide therapy protocol. For medically guided care, see how peptide therapy is supervised at Perfect B in Doral and where a specific peptide fits within a complete treatment plan.
Skip Ahead to the Perfect B Peptide Protocol Tool. See Reconstitution, Daily Units, and Cycle Structure.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
Tesamorelin is not a weight loss drug. It does not suppress appetite, and it does not produce the dramatic scale changes that GLP-1 medications like semaglutide generate. What it does is more specific: it stimulates the pituitary gland to produce more of the body’s own growth hormone, which activates lipolysis in visceral adipose tissue, the deep abdominal fat that wraps around organs and drives metabolic risk. The before and after results patients see on tesamorelin are concentrated in body composition and waist circumference rather than overall body weight.
At Perfect B in Doral, tesamorelin is prescribed as part of a personalized peptide protocol determined at APRN intake. This guide covers what the results trajectory looks like week by week, who the best candidates are, what tesamorelin cannot do, and how it compares to GLP-1 options for patients who are weighing both.

Key Takeaways: Tesamorelin Before and After
- Visceral fat is the primary target: Tesamorelin is the only peptide with FDA approval for reducing visceral adipose tissue. Clinical studies show measurable VAT reduction in treated patients compared to placebo. It works on deep abdominal fat, not subcutaneous fat.
- Results take 8 to 12 weeks to fully develop: Most patients notice early changes in sleep and recovery in weeks 1 to 2. Visible waistline changes typically emerge in weeks 3 to 6. Full body composition results are apparent at 3 months and continue post-cycle.
- It is not a weight loss drug: Tesamorelin shifts fat-to-muscle ratio and reduces visceral fat without the appetite suppression or scale-weight changes of GLP-1 medications. Patients who expect dramatic weight loss will be disappointed. Patients who want improved body composition without GLP-1 side effects are often very well matched.
- Sleep improves early: Many patients report deeper slow-wave sleep within the first two weeks. Better sleep amplifies the benefit because the body’s natural GH pulse occurs during deep sleep, and tesamorelin is timed to amplify that pulse.
- Bedtime timing is critical: Tesamorelin is injected 30 to 90 minutes before sleep and at least 2 to 3 hours after the last meal. This timing aligns the peptide with the natural nocturnal GH release. Late eating or alcohol in the pre-injection window blunts the response.
- 503A compounding pharmacy only: At Perfect B, tesamorelin is sourced from a licensed 503A compounding pharmacy. Research-grade peptides purchased online are not subject to the same pharmaceutical standards and carry meaningfully different risk profiles.
What Tesamorelin Actually Does to Body Composition
Tesamorelin is a growth-hormone-releasing hormone (GHRH) analog. It binds to GHRH receptors on the pituitary gland and stimulates the release of the body’s endogenous growth hormone. It does not introduce synthetic GH into the bloodstream directly; it prompts the pituitary to produce its own. This distinction matters for both safety and physiological fidelity: the GH release follows the body’s own pulsatile pattern rather than producing a sustained supraphysiologic level.
The released GH then activates lipolysis in adipose tissue, with a particular selectivity for visceral adipose tissue (VAT). VAT is the deep fat compartment that surrounds abdominal organs, elevates cardiovascular and metabolic risk markers, and tends to be resistant to diet and exercise interventions that reduce subcutaneous fat. A clinical study published in JAMA demonstrated that tesamorelin produced a statistically significant reduction in visceral adipose tissue compared to placebo, with concurrent improvements in lipid profiles including triglycerides.
Alongside VAT reduction, GH also supports lean muscle mass preservation and protein synthesis. The body composition shift that tesamorelin produces is therefore a two-sided change: visceral fat goes down, lean mass is maintained or improved, and the ratio between fat and muscle in the abdominal region moves in a favorable direction even when total body weight changes only modestly.
Who Is a Good Candidate for Tesamorelin at Perfect B?
Tesamorelin is prescribed off-label at Perfect B for adults who meet specific body composition and health criteria. The APRN intake assesses each patient individually, but the clinical profile that responds best to tesamorelin includes:
- Persistent visceral belly fat that resists diet and exercise: The ideal candidate has implemented consistent nutrition and training but carries stubborn abdominal fat, particularly around the midsection and waist, that has not responded proportionally to overall body fat reduction efforts.
- Patients who want a non-GLP-1 option: Some patients cannot tolerate GLP-1 side effects such as nausea and GI disturbance. Others prefer not to suppress appetite pharmacologically. Tesamorelin offers a body composition pathway that operates through a completely different mechanism without GLP-1 receptor activity.
- Patients in recovery from surgery or reduced activity periods: GH supports muscle protein synthesis and connective tissue remodeling during recovery. Patients who have experienced muscle loss during prolonged rest or post-surgical periods are good candidates for a protocol that protects lean mass while the body rebuilds.
- Adults with metabolic risk markers: Elevated triglycerides, high visceral fat load, and impaired glucose metabolism are all conditions where tesamorelin’s clinical effects on VAT and lipid profiles provide relevant benefit alongside other interventions.
Tesamorelin is not appropriate for patients with active malignancy, uncontrolled diabetes, proliferative retinopathy, or during pregnancy or breastfeeding. The intake consultation at Perfect B specifically screens for these contraindications before any prescription is written.

Tesamorelin Before and After: Week-by-Week Timeline
The tesamorelin results trajectory follows a consistent progression across most patients, though individual speed and magnitude vary based on starting body composition, protocol adherence, sleep quality, and lifestyle factors. The following timeline reflects the clinical pattern documented across provider experiences and the supporting literature.
Weeks 1 to 2: What Changes First
The first changes most patients notice are not in the mirror. They are in sleep quality and recovery. Within the first one to two weeks of the protocol, patients commonly report deeper, more restorative sleep with clearer energy on waking. This reflects the tesamorelin-amplified GH pulse during slow-wave sleep, which also drives tissue repair and recovery processes overnight.
Muscle soreness after training sessions often diminishes in this window. Patients who exercise regularly notice they are recovering faster between sessions. This is not a placebo effect on sleep; the GH pulse that tesamorelin amplifies directly influences the restorative processes that occur during deep sleep, and patients with poor baseline sleep quality often experience the most pronounced early improvement.
Visible body composition changes are not expected in this window. The lipolytic effect on VAT takes more time to accumulate to a visible level. Managing expectations clearly at the start of the protocol is part of how Perfect B’s APRN team sets patients up for a successful three-month commitment.
Weeks 3 to 6: When Patients Notice the Waistline Shift
By weeks three to six, the cumulative lipolytic effect on visceral fat begins to produce visible changes. Patients typically notice a looser waistband, reduced bloating, and a flatter appearance around the lower abdomen. The waist measurement in centimeters often shows the most clinically meaningful change at this stage because visceral fat reduction affects waist circumference more directly than it affects overall body weight.
Patients who train with weights during this period also notice that their progress in the gym becomes easier. GH’s anabolic support at the muscle level means that the same training stimulus produces better lean mass maintenance and often modest strength improvement relative to the pre-protocol baseline.
This is also the window where patients often begin to receive comments from people around them about looking different. The appearance change tends to be perceived as a face change or a general look of being leaner, even when scale weight has not dropped significantly. This reflects the body composition shift rather than weight loss in the conventional sense.
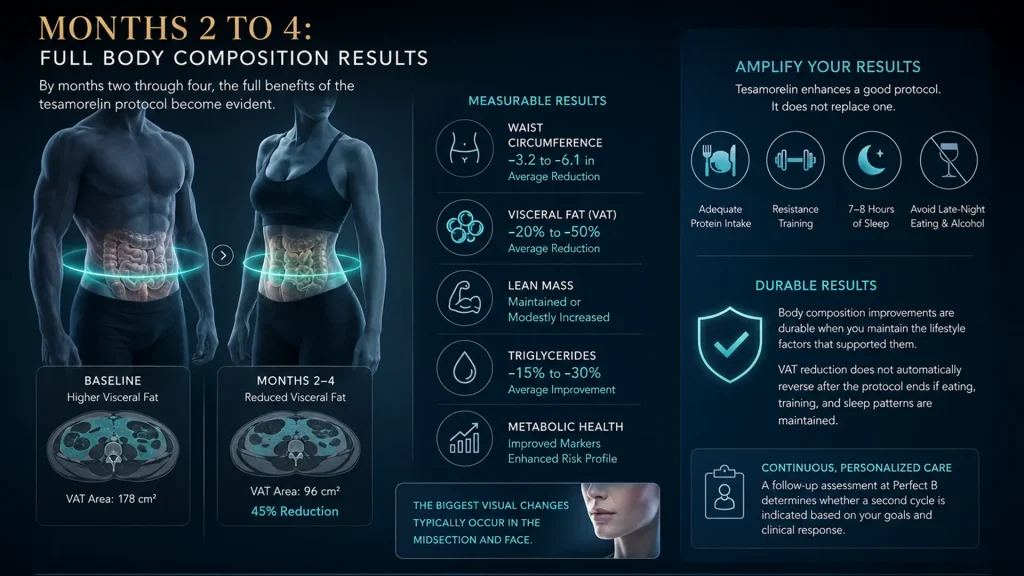
Months 2 to 4: Full Body Composition Results
By months two through four, the full body composition results of the tesamorelin protocol become evident. Visceral fat reduction is now measurable by waist circumference and, in patients who underwent baseline body composition scanning, by direct VAT measurement. Lean mass has been maintained or modestly increased relative to baseline. Metabolic markers including triglycerides have often improved. The face and midsection typically show the most visually apparent changes.
Patients who commit fully to the lifestyle factors that amplify tesamorelin’s effect, specifically adequate protein intake, resistance training, 7 to 8 hours of sleep, and avoidance of late-night eating and alcohol, see results at the higher end of the expected range. The peptide enhances a good protocol; it does not replace one.
After the cycle ends, the body composition improvements made during the protocol are durable if the patient maintains the lifestyle factors that supported them. The VAT reduction does not automatically reverse when the peptide is discontinued, provided eating, training, and sleep patterns are maintained. A follow-up assessment at Perfect B determines whether a second cycle is indicated based on the patient’s remaining goals and clinical response.
What Tesamorelin Does Not Do (Managing Expectations)
Tesamorelin is a specific tool for a specific problem. Patients who arrive at the intake consultation expecting semaglutide-like weight loss results from tesamorelin are not ideal candidates and need honest redirection before starting the protocol.
Tesamorelin does not suppress appetite. It does not reduce overall caloric drive, lower hunger signals, or produce the nausea and food aversion that GLP-1 medications often cause. If appetite management is a primary goal, a GLP-1 protocol is the appropriate clinical choice. Tesamorelin and GLP-1 medications work on entirely different pathways and can be discussed at the intake as complementary or alternative options depending on the patient’s goals and history.
Tesamorelin does not produce significant subcutaneous fat reduction. It targets visceral fat specifically. Patients with primarily subcutaneous fat accumulation on the abdomen, hips, and thighs may see modest improvement in body composition but should not expect the same degree of change that someone with significant visceral fat load will experience.
Tesamorelin does not work well when the lifestyle fundamentals are absent. Without adequate protein, resistance training, consistent sleep, and avoidance of late eating and alcohol near injection time, the GH pulse tesamorelin stimulates is blunted and results are significantly diminished. The protocol requires investment in lifestyle alongside the injection.
Tesamorelin vs GLP-1: Why Some Patients Choose Tesamorelin Instead
The decision between tesamorelin and a GLP-1 protocol depends entirely on what the patient’s primary goal is. They are not substitutes for each other and address different aspects of body composition and metabolic health.
GLP-1 medications produce meaningful overall weight loss by reducing appetite, slowing gastric emptying, and driving a caloric deficit. They are the right choice for patients whose primary goal is total body weight reduction and who need pharmacological support for appetite management. The side effect profile, which includes significant nausea, GI disturbance, and muscle mass loss alongside fat loss, is the tradeoff.
Tesamorelin targets the specific metabolic problem of visceral fat without touching appetite or total caloric balance. It preserves muscle mass while reducing VAT, improves sleep quality, and supports recovery. Patients who have already achieved general weight loss through GLP-1 or lifestyle but carry residual visceral fat are strong candidates for adding tesamorelin to specifically address that compartment. Patients who cannot tolerate GLP-1 side effects and want a body composition intervention without appetite suppression are also well matched to tesamorelin.
For a broader comparison of peptide options vs GLP-1 medications at Perfect B, see our guide on peptides for weight loss vs Ozempic.
How to Maximize Your Results: What to Pair With Tesamorelin
Tesamorelin amplifies a good protocol. The patients who see the best before and after results are those who pair the injection with consistent lifestyle inputs that support GH release and body composition improvement.
- Protein intake: Aim for 1.6 to 2.0 grams per kilogram of body weight per day, distributed across meals of 25 to 40 grams per sitting. Protein supports muscle protein synthesis and prevents the lean mass loss that can accompany fat loss.
- Resistance training: Two to three short sessions per week using compound movements produce the training signal that GH then amplifies. Resistance training does not need to be high-volume to produce meaningful results when paired with tesamorelin; consistency and progressive overload matter more than session length.
- Post-meal walks: 10 to 20 minutes of walking after lunch and dinner blunts the glucose and triglyceride spikes from meals, reducing the substrate that would otherwise be stored as visceral fat. This is a low-effort intervention with meaningful metabolic impact.
- Sleep window: Protecting 7 to 8 hours of sleep with consistent bed and wake times maximizes the slow-wave sleep phase where tesamorelin’s amplified GH pulse has its greatest effect. Erratic sleep schedules significantly reduce results.
- Pre-injection fasting window: Inject at least 2 to 3 hours after the last meal and avoid alcohol in the evening before injection. Insulin from a recent meal and alcohol both suppress GH release, blunting the tesamorelin response.

503A Compounding vs Research-Grade Tesamorelin
Tesamorelin is not available as a commercial injectable outside the FDA-approved indication for HIV-associated lipodystrophy. For off-label clinical use, it must come from a licensed 503A compounding pharmacy that manufactures under pharmaceutical-grade conditions with documented sterility testing, potency verification, and third-party quality standards.
Research-grade tesamorelin sold online is classified for laboratory use, not human administration. It is produced without the manufacturing standards, sterility requirements, or potency documentation that a licensed pharmacy must maintain. The difference between clinic-grade and research-grade peptides is not theoretical: it affects the actual peptide content, sterility, contamination risk, and the accountability chain that protects the patient. At Perfect B, all tesamorelin is sourced from licensed 503A compounding pharmacies. For a full explanation of why this distinction matters, see our guide to peptide treatment at Perfect B in Doral.
Frequently Asked Questions About Tesamorelin Before and After
1. How long does tesamorelin take to work?
The first changes most patients notice are in sleep quality and recovery speed, typically within the first one to two weeks. Visible waistline and body composition changes emerge in weeks three to six as the cumulative lipolytic effect on visceral fat accumulates. Full results from a complete cycle are apparent at the three-month mark and continue to develop for several weeks after the cycle ends.
2. What are the results of tesamorelin at 4 weeks?
At four weeks, most patients are noticing clear improvements in sleep quality, morning energy, and gym recovery. Early waistline changes are beginning to emerge, often visible as a tighter appearance around the lower abdomen. The full body composition shift is still developing at this stage. Patients who have also implemented protein intake and resistance training alongside the injection typically see the most progress at the four-week mark.
3. Does tesamorelin remove belly fat?
Tesamorelin specifically targets visceral belly fat, the deep abdominal fat that surrounds organs. It is not as effective for subcutaneous belly fat, which sits above the muscle layer and has a different hormonal and metabolic profile. For patients carrying primarily visceral fat, tesamorelin’s clinical evidence for VAT reduction is strong. The JAMA clinical study demonstrated statistically significant visceral adipose tissue reduction in treated patients.
4. Does tesamorelin make your face puffy?
Temporary water retention is a possible early side effect of tesamorelin in some patients as GH levels increase. This can produce mild puffiness, particularly in the face and extremities, in the first few weeks of the protocol. For most patients, this resolves as the body adapts to the new hormonal environment. If puffiness persists beyond the adjustment period, the APRN reviews the protocol and may adjust the dose or timing.
5. Can tesamorelin be combined with other peptides?
Yes. Tesamorelin is commonly combined with ipamorelin, which amplifies the GH secretagogue effect through a complementary pathway. This bedtime combination strengthens the nocturnal GH pulse without increasing cortisol or prolactin. At Perfect B, combination protocols are determined at the intake consultation based on the patient’s goals and health profile. See our full tesamorelin dosage protocol guide for details on how the protocol is structured.
6. How long should you stay on tesamorelin?
At Perfect B, tesamorelin protocols are structured in 3-month cycles followed by a reassessment. Some patients achieve their body composition goals in a single cycle and do not require a second. Others with more significant visceral fat loads or additional metabolic goals continue for a second cycle after the follow-up assessment confirms it is appropriate. Running tesamorelin indefinitely without cycle breaks and reassessment is not part of the protocol at Perfect B.
7. Is tesamorelin better than GLP-1 for belly fat?
For visceral fat specifically, tesamorelin has a more targeted mechanism. GLP-1 medications produce overall fat loss through caloric deficit driven by appetite suppression, which reduces both subcutaneous and visceral fat proportionally. Tesamorelin targets visceral fat directly through GH-driven lipolysis without affecting appetite or total body weight substantially. For a patient whose primary concern is visceral fat and who does not need appetite suppression, tesamorelin is the more specific tool. For a patient who needs to lose significant overall body weight, GLP-1 medications are typically more appropriate.
8. What is the difference between tesamorelin research-grade and compounded?
Research-grade tesamorelin is classified for laboratory use only and is manufactured without the pharmaceutical standards required for human administration. Compounded tesamorelin from a licensed 503A pharmacy is manufactured under pharmaceutical-grade conditions with sterility testing, potency verification, and documented quality control. At Perfect B, all tesamorelin is sourced from licensed 503A compounding pharmacies. The difference in safety, purity, and accountability is significant.
Closing: The Tesamorelin Before and After Is a Body Composition Story, Not a Weight Loss Story
The patients who experience the most satisfying before and after results on tesamorelin are those who understand what they are signing up for: a targeted intervention against visceral fat that preserves muscle, improves metabolic markers, and enhances sleep and recovery over a three-month cycle. It is not a shortcut to a lower number on the scale. It is a clinical tool for a specific body composition goal that diet, exercise, and GLP-1 medications do not address with the same precision.
At Perfect B in Doral, the intake consultation is where the right patients are identified, the protocol is built, and the expectations are set correctly from the start. Tesamorelin works when it is matched to the right patient and paired with the right lifestyle inputs. For patients who fit the profile, the before and after at three months reflects something that most other interventions cannot produce: a measurable shift in the deep abdominal fat compartment that drives long-term metabolic risk.
For more on how tesamorelin fits into Perfect B’s peptide framework, see our tesamorelin vs sermorelin comparison and the complete tesamorelin dosage protocol guide.
📍 Perfect B | 8200 NW 41st St, Suite 100, Doral, FL 33166
📞 (786) 502-2260


