

6 Questions. One Personalized Peptide Protocol. Zero Guesswork.
Instead of guessing which peptide is right for you, answer 6 short questions in our peptide guide and see the protocols real Perfect B patients with your goals are following.
→ Take the 6-question peptide guide at peptides.perfectb.com
Perfect B, Doral Fl. | 05.28.26 | 10 min read.
This content is for educational purposes only and does not constitute medical advice. Peptide therapy involves prescription compounds that require a licensed medical provider, clinical evaluation, and laboratory monitoring. Results vary by individual. Consult a qualified provider before beginning any peptide protocol. For the bigger picture, read how medically supervised peptide therapy at Perfect B in Doral works and how each protocol fits a complete, monitored plan.
What Peptides Actually Do for Muscle Growth
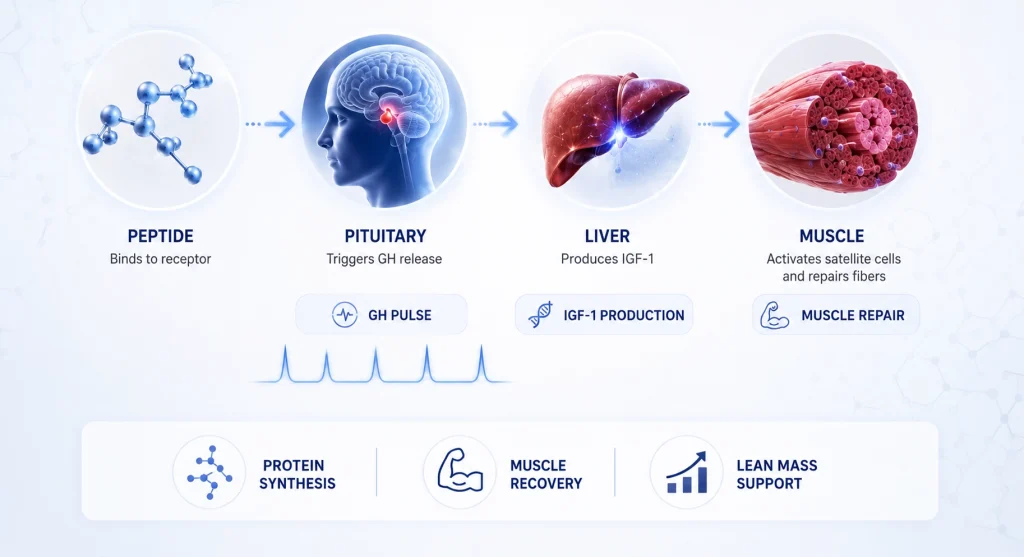
Peptides for muscle growth work through one primary axis: the growth hormone and insulin-like growth factor 1 pathway. When the right peptide binds to its receptor, it signals the pituitary gland to release endogenous growth hormone. That GH pulse then triggers IGF-1 production in the liver, which travels to skeletal muscle, activates satellite cells, and drives protein synthesis, the process through which muscle fibers repair and hypertrophy after training stress.
This is not the same as injecting synthetic human growth hormone. Growth hormone secretagogues, the class of peptides used in clinical practice for muscle growth and body recomposition, stimulate your own pituitary to release GH in a pulsatile pattern that mirrors the body’s natural rhythm. That distinction matters clinically because it preserves the feedback loop that governs GH secretion, reducing the risk of the side effects associated with exogenous HGH administration at therapeutic doses.
The peptides that actually deliver results in this context are CJC-1295, Ipamorelin, Tesamorelin, BPC-157, and TB-500. Each one addresses a different part of the muscle growth and recovery equation. No single peptide is a complete solution on its own. The protocols that produce the most consistent body recomposition outcomes at supervised clinics use at least two of them in combination.
Key Takeaways on Peptides for Muscle Growth
- GH secretagogues drive the muscle growth response: CJC-1295 and Ipamorelin work by stimulating the pituitary to release growth hormone in a physiological pulsatile pattern, which drives IGF-1 production and protein synthesis in skeletal muscle.
- Recovery is half the equation: BPC-157 and TB-500 do not directly stimulate GH, but they accelerate tendon, ligament, and muscle tissue repair, allowing patients to train with greater frequency and intensity without connective tissue breakdown limiting progress.
- Peptides are not steroids: GH secretagogues work within the body’s own hormonal feedback system. They do not suppress natural testosterone production, cause liver toxicity, or produce the androgenic side effects associated with anabolic steroid use.
- Prescription and lab work come first: Peptide therapy for muscle growth requires a medical evaluation, baseline labs including IGF-1 and fasting glucose, and ongoing monitoring. It is not a supplement that can be self-administered from an online vendor.
- Timeline is 8 to 12 weeks minimum: The muscle growth and body composition changes from peptide therapy develop over months, not weeks. Patients who see the most consistent results are those who combine peptide protocols with structured resistance training and adequate protein intake.
Not Sure Which Peptide Protocol Fits Your Muscle Recovery Goal? See What Perfect B Patients With Similar Goals Are Running.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
The Four Peptides That Matter for Muscle Growth at a Medical Clinic
Most online content about the best peptides for muscle growth lists every compound ever tested in a rodent model. A medical clinic operates from a different framework: which peptides for building muscle have sufficient human evidence, prescribable status, known safety profiles, and practical relevance for the patients coming through the door. At a supervised practice in South Florida, that narrows the list considerably.
CJC-1295 paired with Ipamorelin
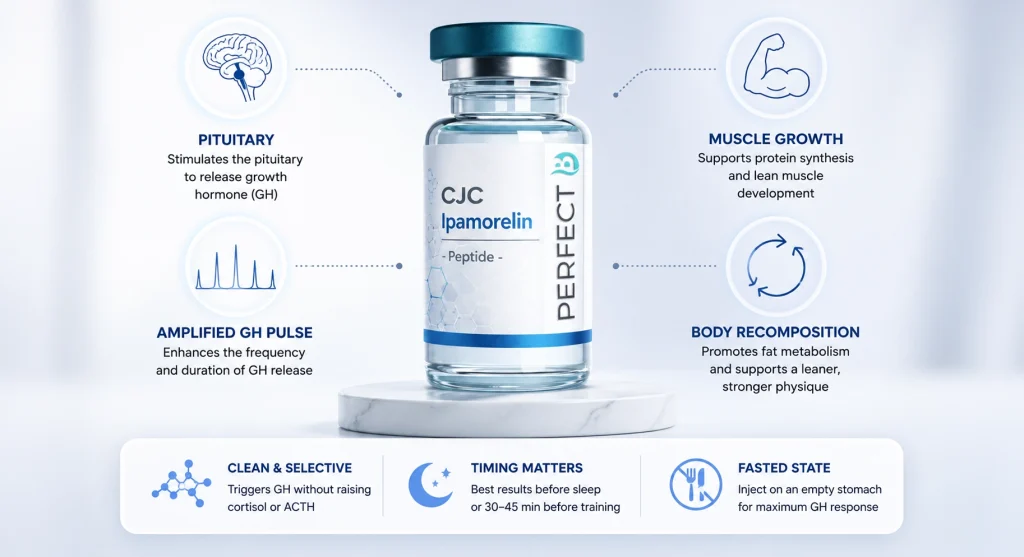
This is the most widely used growth hormone secretagogue combination in clinical peptide practice. CJC-1295 is a synthetic analogue of growth hormone-releasing hormone that extends the half-life of the GH signal significantly compared to native GHRH. Ipamorelin is a selective ghrelin receptor agonist that stimulates GH release through a complementary pathway without producing the cortisol and ACTH elevation seen with older secretagogues. Together, they create a synergistic GH pulse that is larger than either compound produces alone and more physiologically similar to the natural nocturnal GH release pattern.
The clinical relevance for peptides bodybuilding and muscle building applications is that the amplified GH pulse raises IGF-1, which drives muscle protein synthesis and supports the preferential use of fat for energy during training. Our complete clinical overview of CJC-1295 and Ipamorelin at Perfect B explains how this combination works at the receptor level, what the injection protocol looks like, and what patients typically experience over a 3-month cycle.
Tesamorelin
Tesamorelin is the most rigorously studied GH-releasing peptide available, with FDA approval for a specific indication and a significant body of published clinical trial data. It is a stabilized synthetic form of GHRH that stimulates the pituitary more strongly than endogenous GHRH alone. For patients focused on body recomposition, particularly visceral fat reduction alongside lean mass preservation, Tesamorelin offers a clinical evidence base that other peptides in this category cannot match. The full clinical breakdown of how Tesamorelin works, who it benefits most, and how it compares to CJC-1295/Ipamorelin for different patient goals is covered in our Tesamorelin treatment guide at Perfect B in Doral.
BPC-157
BPC-157 is a synthetic pentadecapeptide derived from a gastric protein. Its mechanism for muscle growth support is indirect: it accelerates the repair of tendons, ligaments, and muscle tissue that would otherwise represent the rate-limiting factor in training progression. Patients who push training frequency and intensity are limited not by motivation but by connective tissue recovery. BPC-157 reduces that limitation by accelerating fibroblast recruitment, increasing collagen synthesis, and modulating inflammation in ways that translate to faster recovery between sessions. The clinical profile of BPC-157, including how it compares to TB-500 and when the two are combined at our Doral clinic, is in our complete BPC-157 guide.
TB-500 (Thymosin Beta-4 fragment)
TB-500 is a synthetic analogue of the naturally occurring peptide Thymosin Beta-4. Where BPC-157 targets connective tissue repair with site specificity, TB-500 has a broader systemic recovery profile. It promotes actin polymerization, supports angiogenesis in healing tissue, and reduces systemic inflammatory markers that accumulate with consistent high-volume training. For patients who run both BPC-157 and TB-500 together, the combination addresses tissue repair from two distinct mechanistic angles simultaneously.
Why CJC-1295 and Ipamorelin Is the Core of Every Muscle Growth Protocol
Among all the peptides used for muscle gain and body recomposition, CJC-1295 paired with Ipamorelin is the combination most consistently prescribed at medical clinics with established peptide programs. Several factors explain why it functions as the core of most protocols.
The selectivity of Ipamorelin is clinically significant. Early GH secretagogues like GHRP-2 and GHRP-6 produced GH release but also elevated cortisol and ACTH, which counteract the anabolic environment you are trying to create with peptides for muscle building. Ipamorelin releases GH without those hormonal side effects, making it cleaner as a clinical tool. The study published in the European Journal of Endocrinology characterizing Ipamorelin as a selective growth hormone secretagogue with a favorable side effect profile compared to earlier GHRP compounds established the mechanistic basis for preferring it over older alternatives.
The timing protocol matters as much as the compound selection. CJC-1295/Ipamorelin is most commonly administered subcutaneously before sleep, when the natural GH pulse is largest, or approximately 30 to 45 minutes before training. Fasted administration maximizes the GH response because elevated insulin from a recent meal suppresses GH secretion. At our clinic in Doral, FL, patients who follow the timing protocol precisely consistently report better outcomes than those who inject at inconsistent times or around large meals.
BPC-157 and TB-500: Why Recovery Is Half the Muscle Growth Equation
The rate-limiting factor in muscle growth for most trained individuals is not the amount of GH or IGF-1 circulating at any given time. It is the ability of connective tissue, tendons, ligaments, and the extracellular matrix surrounding muscle fibers to tolerate the mechanical demands of progressive overload. When training stress exceeds what connective tissue can recover from between sessions, training volume drops, injuries accumulate, and the anabolic stimulus from the GH peptides cannot be fully converted into muscle protein accretion.
BPC-157 addresses this directly. Its mechanism involves upregulation of growth factor expression in tendons and ligaments, promotion of collagen synthesis, and acceleration of the fibroblast recruitment that rebuilds connective tissue architecture. Preclinical research on BPC-157 shows consistent findings across tendon, muscle, and ligament models. A 2021 review in Nutrients examining the relevance of bioactive peptides in sports nutrition, including their roles in tissue repair, muscle protein synthesis, and recovery from exercise-induced damage supports the mechanistic rationale for including repair-focused peptides alongside GH secretagogues in performance-oriented protocols.
TB-500 complements BPC-157 by operating systemically rather than site-specifically. It is particularly relevant for patients whose training produces diffuse connective tissue stress across multiple joints simultaneously, which is common in athletes running compound movements at high volumes. In South Florida, where year-round outdoor training is the norm and patients often maintain high training frequency without seasonal deload periods, the recovery stack of BPC-157 plus TB-500 is one of the most practical additions to a GH secretagogue protocol.
Peptides vs Steroids: What the Clinical Difference Actually Is
Patients researching peptides for muscle growth frequently encounter content that conflates GH secretagogues with anabolic steroids. The mechanisms are fundamentally different, and that difference has significant clinical implications.
Anabolic-androgenic steroids work by binding directly to androgen receptors, producing androgenic effects alongside anabolic ones. This means testosterone suppression through the hypothalamic-pituitary-gonadal axis, potential liver stress with oral formulations, lipid dysregulation, and androgenic effects in both sexes. The anabolic gains are real but come with a hormonal trade that requires post-cycle management.
GH secretagogues work through an entirely separate axis. They do not bind androgen receptors. They do not suppress natural testosterone production. They do not produce androgenic effects. Their primary hormonal action is on the somatotropic axis: more GH, more IGF-1, more protein synthesis, and more favorable partitioning between fat and lean mass. The side effect profile at clinical doses is significantly different, and the recovery profile after stopping peptides does not involve the endocrine disruption that post-cycle therapy is designed to address in steroid users.
This does not mean GH secretagogues are without considerations. Elevated IGF-1 has implications for patients with certain health histories. Blood glucose monitoring is appropriate because growth hormone can transiently affect insulin sensitivity. Any patient with active malignancy, uncontrolled metabolic disease, or a history of endocrine tumors is not a candidate for GH-stimulating peptide therapy. The clinical evaluation before prescribing exists precisely to identify these contraindications.
Body Recomposition vs Pure Muscle Gain: Which Protocol Fits Your Goal
Most patients who come in asking about peptides for muscle growth are not competitive bodybuilders trying to maximize absolute mass. They are physically active adults who want to add lean tissue, reduce body fat, and improve overall body composition simultaneously. This body recomposition goal requires a different framing than pure muscle-building protocols.
For body recomposition, the combination of a GH secretagogue with AOD 9604, a fragment of human growth hormone that drives lipolysis through beta-3 adrenergic receptors without affecting muscle anabolism, is worth considering for patients whose primary concern is concurrent fat loss and muscle preservation. CJC-1295/Ipamorelin drives the anabolic side of the equation while AOD 9604 addresses the lipolytic side through a complementary mechanism that does not interfere with GH receptor signaling.
For patients primarily focused on peptides for muscle gain with fat loss as a secondary outcome, CJC-1295/Ipamorelin or Tesamorelin alone is typically sufficient, with the understanding that the elevated IGF-1 environment naturally supports more favorable nutrient partitioning. Adding BPC-157 and TB-500 to either protocol extends the training tolerance that determines how much of the hormonal signal actually converts to muscle tissue.
See how peptides for muscle growth fit into a real supervised protocol at Perfect B.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
Who Gets the Most Out of Peptide Therapy for Muscle Growth
Peptide therapy for muscle growth is not universally appropriate, and the patients who respond best share several consistent characteristics that emerge clearly when you look at outcomes across a supervised clinical practice.
- Already training consistently before starting: Patients at our clinic in Doral who see the strongest lean mass response to CJC-1295/Ipamorelin are those who were already training 3 or more times per week before their first injection. The peptides amplify a training stimulus that is already present. They do not replace it.
- Protein intake is already adequate: GH-stimulated protein synthesis requires dietary protein as substrate. Patients eating at or below 0.7 grams per pound of bodyweight do not have the raw material to convert the anabolic signal into muscle tissue. Nutritional intake must be addressed alongside the peptide protocol.
- Age 30 and older with declining GH pulsatility: Natural GH release declines significantly after the mid-20s. Patients in their 30s, 40s, and 50s who have maintained training intensity but notice slower recovery, reduced lean mass, and more difficult fat loss are the population that responds most predictably to GH secretagogue therapy.
- No significant metabolic contraindications: Active malignancy, uncontrolled insulin resistance, or significant thyroid disease can alter both the risk-benefit calculation and the expected response. Lab work before prescribing identifies which patients are appropriate candidates.
- Realistic timeline expectations: Patients who expect visible muscle changes within 2 to 3 weeks are typically disappointed. Patients who understand that the GH-IGF-1 cycle operates on a 4 to 8 week minimum timeline, and that cumulative results build over 3 to 6 months of consistent protocol adherence, are the ones who complete a full cycle and achieve meaningful body composition change.
The Realistic Timeline: Weeks 1 Through 12 and Beyond
Understanding the physiological timeline of peptide therapy for muscle growth prevents the two most common errors: abandoning a protocol before it has had time to work, and expecting steroid-like speed of change from a compound that operates through the body’s own hormonal architecture. The progression is real but measured.

Weeks 1 through 3 are the establishment phase. IGF-1 levels begin to rise as the GH pulse amplifies with each injection. Most patients notice improved sleep quality and faster recovery between sessions before they see any visible body composition change. This is because GH’s effect on sleep architecture is one of its most consistent early signs, and connective tissue repair accelerates before lean mass becomes measurable.
Weeks 4 through 6 are when the first physical changes typically emerge. Patients report a reduction in post-workout soreness duration, some initial visible changes in muscle fullness from improved glycogen storage, and the beginning of body fat reduction around the abdomen where GH-driven lipolysis preferentially acts on visceral fat stores. Training performance often improves at this stage because recovery is genuinely faster.
Weeks 8 through 12 are where consistent body recomposition becomes measurable. Lean mass gains of 2 to 4 pounds over a 12-week cycle at 300 mcg CJC-1295/Ipamorelin daily, combined with adequate protein intake and structured training, are a realistic clinical expectation. Body fat reduction of 1 to 3 percent of total body fat over the same period is consistent with published data on GH secretagogue effects on body composition. These numbers are smaller than anabolic steroid outcomes, but they come without the corresponding hormonal disruption or post-cycle requirements.
Beyond 12 weeks, cumulative compounding occurs. Each cycle builds on the tissue changes from the previous one, and patients who maintain protocol adherence over 6 to 12 months of treatment typically report the most meaningful transformation in how their body responds to training.
See what patients with similar muscle recovery goals are running at Perfect B.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
Peptides for Muscle Growth in Miami: What Supervised Therapy Looks Like at Our Clinic
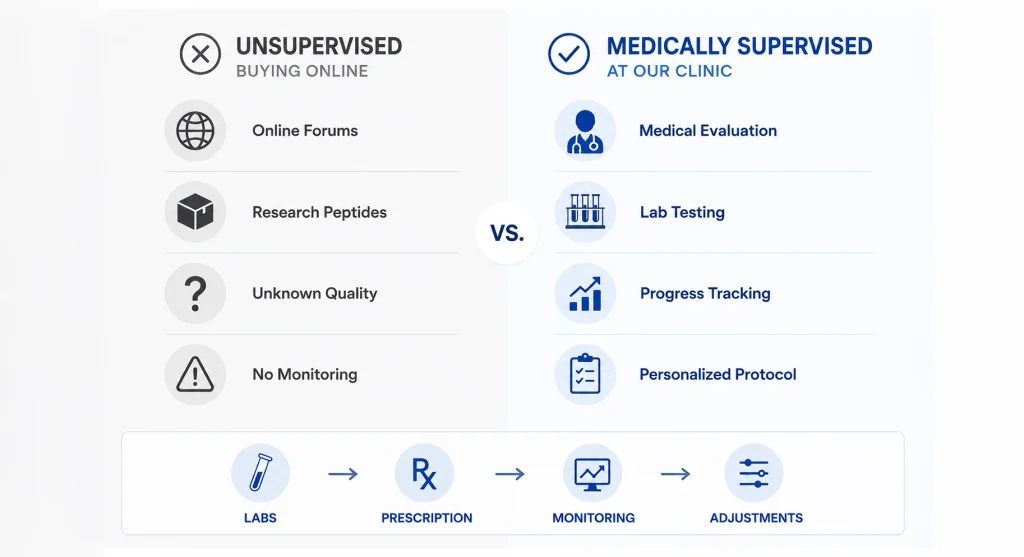
The conversation about peptides for muscle growth in the Miami area has largely happened online, through forums, supplement sites, and social media accounts run by people selling research-grade compounds that bypass prescription requirements entirely. The patient who comes to a medical clinic has usually already read those sources and arrives with one central question: is there a version of this that is actually supervised?
At Perfect B in Doral, the peptide therapy program for muscle growth and body recomposition starts with a clinical intake and baseline lab panel. We check IGF-1, fasting glucose, and a relevant metabolic panel before prescribing anything. This is not a formality. IGF-1 baseline matters because it tells us where your somatotropic axis is starting from and helps calibrate which protocol and dosing approach is appropriate. Fasting glucose matters because GH can affect insulin sensitivity transiently, and a patient with undiagnosed prediabetes needs a different conversation before starting a GH secretagogue than a metabolically healthy patient does.
The prescription is written for compounded CJC-1295/Ipamorelin or Tesamorelin through a licensed compounding pharmacy that meets USP standards. The patient receives injection training, a written protocol with timing and dosing instructions, and a follow-up schedule. IGF-1 is rechecked at the 6 to 8 week mark to confirm the expected response. Adjustments to dosing or compound selection happen based on lab data and reported patient experience, not according to a fixed protocol applied the same way to every patient.
Frequently Asked Questions
1. What are the best peptides for muscle growth?
At a supervised medical clinic, the most clinically supported option for muscle growth and body recomposition is CJC-1295 paired with Ipamorelin. This combination produces synergistic GH release through complementary receptor pathways, drives IGF-1 production that stimulates muscle protein synthesis, and does so without the cortisol and ACTH elevation seen with older growth hormone secretagogues. Tesamorelin is a well-studied alternative with a stronger clinical evidence base from formal trials. For recovery support alongside a GH secretagogue, BPC-157 and TB-500 address the connective tissue bottleneck that limits training frequency and intensity.
2. How long do peptides take to work for muscle building?
The first measurable changes from peptide therapy for muscle gain typically emerge at the 4 to 6 week mark. Improved sleep quality and reduced recovery time are usually the first signs, followed by visible changes in muscle fullness and the beginning of body fat reduction around weeks 4 through 6. Meaningful lean mass gains and body recomposition become consistently measurable at the 8 to 12 week mark. Most patients who complete a full 12-week protocol and maintain adequate protein intake and training consistency report 2 to 4 pounds of lean mass gained and a 1 to 3 percent reduction in body fat percentage.
3. Are peptides for muscle growth safe?
When prescribed and monitored by a licensed medical provider, GH secretagogue peptides like CJC-1295/Ipamorelin and Tesamorelin have a well-characterized safety profile in the published literature. They do not suppress natural testosterone, do not cause liver toxicity, and do not produce androgenic side effects. The main clinical monitoring points are IGF-1 levels and fasting glucose, as GH can transiently affect insulin sensitivity. Patients with active malignancy, uncontrolled metabolic disease, or a history of endocrine tumors are not appropriate candidates. Self-administered research peptides from online vendors bypass these safeguards entirely, which is why the risk profile of supervised therapy and unsupervised use are not comparable.
4. What is the difference between peptides and steroids for muscle growth?
The mechanism is fundamentally different. Anabolic steroids work by binding androgen receptors directly, producing muscle growth alongside androgenic effects, testosterone suppression, and potential liver stress that require post-cycle management. GH secretagogue peptides work through the somatotropic axis, stimulating the pituitary to release your own growth hormone in a physiological pattern. They do not suppress natural testosterone production, do not bind androgen receptors, and do not require post-cycle therapy. The muscle growth is more gradual, but it develops without the hormonal disruption associated with androgen-based compounds.
5. Can peptides help with body recomposition, not just muscle gain?
Yes. This is one of the most clinically relevant applications of GH secretagogue peptides. The elevated IGF-1 environment drives protein synthesis and lean mass accretion while the GH-mediated lipolysis preferentially mobilizes visceral and subcutaneous fat, particularly in the abdominal region. For patients who want to add lean tissue and reduce fat simultaneously, rather than bulk and cut in separate cycles, GH secretagogues create the hormonal environment that makes concurrent recomposition more achievable than it would be with training and nutrition alone.
6. Do I need to be a bodybuilder to benefit from peptides for muscle growth?
No. The majority of patients at medical clinics seeking peptide therapy for muscle growth are active adults in their 30s, 40s, and 50s who train consistently but have noticed slower recovery, more difficulty maintaining lean mass, and reduced response to the training stimuli that worked well for them a decade earlier. These are the patients for whom GH secretagogue therapy most reliably addresses the physiological gap between training intention and training outcome. Competitive bodybuilders represent a small fraction of the population that benefits from supervised peptide therapy.
7. What labs are checked before starting peptide therapy for muscle growth?
A responsible medical practice checks IGF-1 at baseline, fasting glucose, and a general metabolic panel before prescribing any GH secretagogue. IGF-1 establishes the starting point of the somatotropic axis and guides protocol selection and dosing. Fasting glucose is checked because GH can transiently affect insulin sensitivity, and a patient with prediabetes or undiagnosed metabolic syndrome requires a different clinical conversation. Testosterone and thyroid function may also be relevant depending on the patient’s history and symptoms. Lab results are reviewed at the 6 to 8 week follow-up to confirm expected response and adjust the protocol if needed.
Closing: The Clinical Case for Supervised Peptide Therapy in a Training-Focused Patient
The question is not whether peptides for muscle growth work. The clinical evidence for GH secretagogues driving lean mass accretion, improving body composition, and supporting recovery is substantive enough that it does not require overselling. The question that matters clinically is whether a given patient is a good candidate, what the right protocol looks like for their specific goals and lab results, and whether they have access to a supervised framework that can catch the small number of patients for whom these compounds are not appropriate before they start rather than after.
The South Florida market for peptide therapy is large and largely unsupervised. Patients in the Miami area have no shortage of online vendors, telemedicine platforms with minimal intake standards, and gym networks that provide access to research peptides outside any medical framework. What is harder to find is a clinic that combines the peptide therapy knowledge base with the clinical infrastructure to do it correctly: real labs, real prescriptions, real follow-up, and a provider who has seen enough patients on these protocols to recognize what a normal response looks like and what requires attention. That is what the program at Perfect B in Doral represents for patients who want to take this seriously.
- 📍 Visit us at Perfect B, Doral FL, serving Miami and South Florida patients seeking performance and muscle growth peptide therapy.
- 📞 Call or message us at (786) 502-2260 to schedule your peptide consultation for muscle growth with a licensed medical provider.


