

Perfect B, Doral Fl. | 06.03.26 | 9 min read.
This content is for educational purposes only. It does not constitute medical advice and is not a substitute for evaluation by a licensed medical provider. CJC-1295/Ipamorelin is a prescription peptide that requires clinical supervision. Do not use this information to self-administer or self-diagnose. Contact Perfect B at (786) 502-2260 to schedule a clinical evaluation. If you are exploring this, it helps to see how peptide therapy is supervised at Perfect B in Doral and where a specific peptide fits within a complete treatment plan. For more on this, see our guide to IGF-1 Blood Test: Why Peptide Therapy Starts With Labs, and how it is evaluated and treated at Perfect B in Doral.
Key Takeaways: What Women Need to Know About CJC-1295/Ipamorelin
- Growth hormone production starts declining at 35, not at menopause. GH pulse frequency in women is regulated by estrogen, which begins shifting during perimenopause, often a decade before full menopause arrives.
- CJC-1295 and Ipamorelin work through two separate receptor pathways. Combining them produces a synergistic GH pulse that neither peptide achieves independently, which is why the stack outperforms either alone.
- Sleep quality is typically the first noticeable change. Women using cjc 1295 ipamorelin for women report deeper, more restorative sleep within 2 to 3 weeks, before body composition changes become visible.
- Dosing for women is not a scaled-down version of male protocols. Women clear peptides differently due to hormonal physiology, and the protocol at Perfect B adjusts for hormonal baseline, cycle status, and lab results.
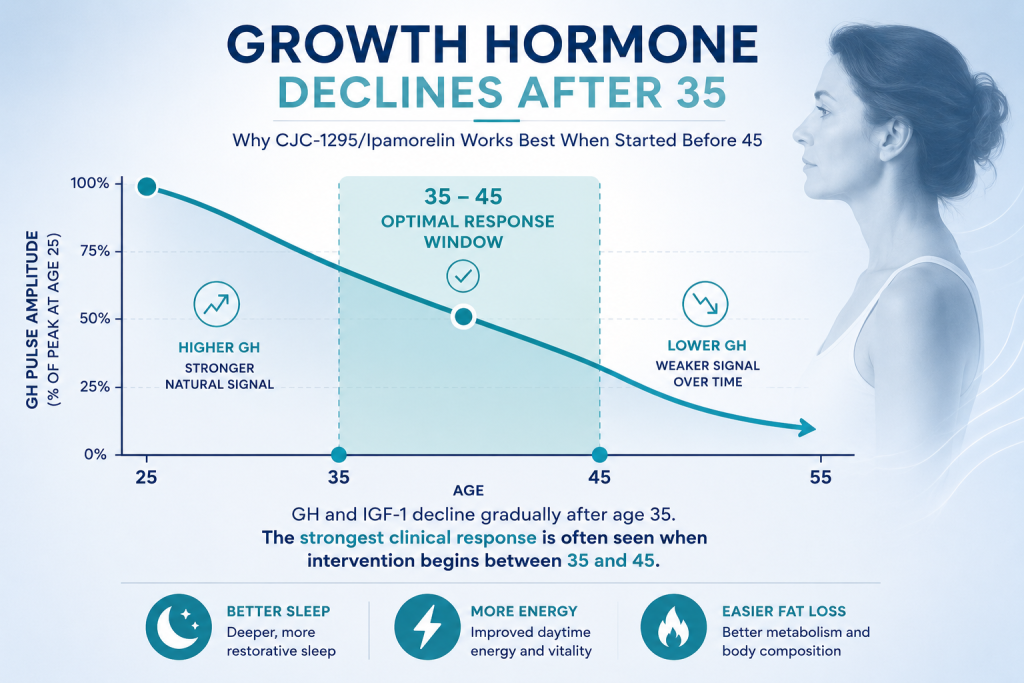
- The optimal intervention window is 35 to 45. GH has dropped enough to produce symptoms, but enough pituitary responsiveness remains for strong clinical results during this window.
What Happens to Women’s Growth Hormone After 35?
Growth hormone in women is not a stable background signal. It pulses, primarily during deep sleep, and those pulses are regulated in part by estrogen. When estrogen levels begin the gradual perimenopause transition in the mid-to-late 30s, GH pulse amplitude and frequency decline alongside it. Women often notice the downstream effects years before connecting them to growth hormone: sleep becomes lighter, recovery from exercise takes longer, body fat shifts toward the abdomen, and skin begins losing density.
The clinical literature confirms that women have higher baseline GH secretion than men during their reproductive years, partly because estrogen stimulates GH release from the pituitary. This higher baseline is protective. When it starts to drop, the change is not gradual across decades. It is a measurable shift that correlates with perimenopause onset, not with menopause itself. By the time a woman reaches full menopause, she has already been losing GH pulse frequency for 10 to 15 years.
Why Perimenopause Is the Inflection Point, Not Menopause
Perimenopause begins earlier than most women expect, often in the early-to-mid 30s as a gradual, subclinical process. A woman who feels that her body has “changed” after 35 without a clear explanation is often correct, and the GH axis is one of the primary reasons. The fatigue is real. The change in body composition is real. Waiting for a menopause diagnosis before addressing it means waiting through the years when intervention is most effective.
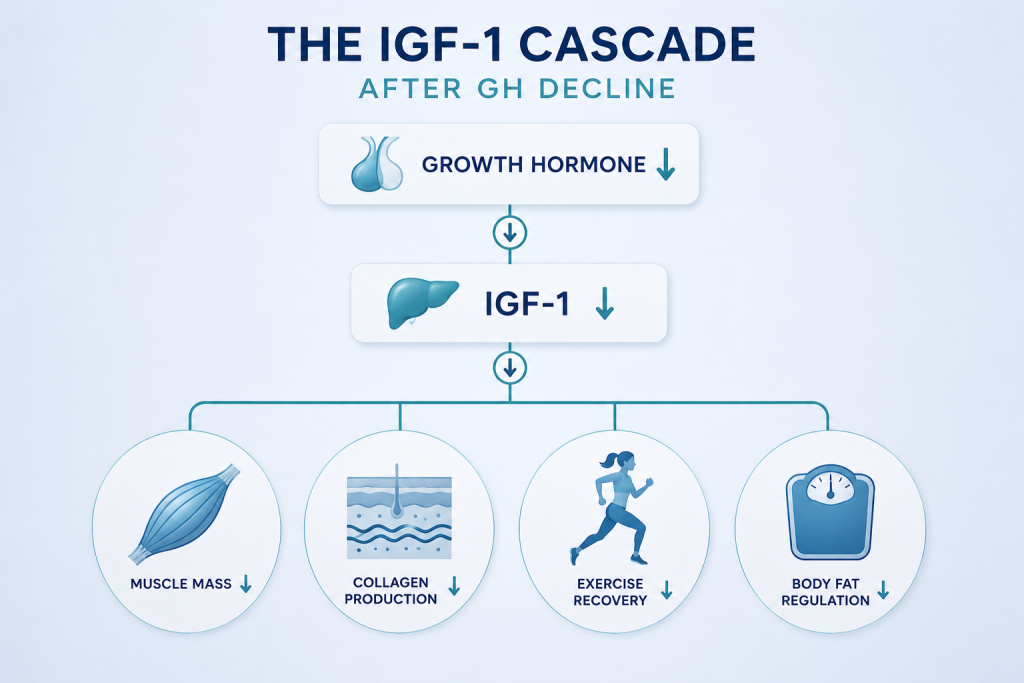
The IGF-1 Cascade That Follows GH Decline
When GH declines, IGF-1 (insulin-like growth factor 1) follows. IGF-1 is the primary mediator of GH’s downstream effects in tissue, muscle, bone, and skin. Lower IGF-1 means reduced lean muscle preservation, slower collagen synthesis, impaired exercise recovery, and progressive changes to how the body partitions fat versus muscle. Measuring IGF-1 at baseline is the first step in the evaluation at Perfect B, because it tells us where on that decline curve a patient currently is.
What Are CJC-1295 and Ipamorelin, and Why Does the Combination Matter?
CJC-1295 is a growth hormone-releasing hormone (GHRH) analog. It binds to GHRH receptors in the pituitary and stimulates growth hormone secretion. Ipamorelin is a growth hormone-releasing peptide (GHRP). It binds to ghrelin receptors in the pituitary through a completely separate mechanism. Ipamorelin is notable because, unlike earlier GHRPs, it produces GH release without significantly elevating cortisol or prolactin. These were the side effect problems that made older GHRPs less clinically appealing for women. For a full overview of how both peptides work independently, our guide to what CJC-1295/Ipamorelin is and how it works at a clinical level covers the mechanism in detail.
Why the Combination Produces a Different Result Than Either Alone
When CJC-1295 and Ipamorelin are administered together, they activate two separate pathways to GH release simultaneously. The result is a synergistic pulse that is significantly larger than either peptide alone, while still being a physiological pulse rather than a pharmacological spike. The pituitary responds as if the body is producing GH naturally, which means the downstream IGF-1 response and tissue effects follow normal biological patterns. This is clinically important because a physiological pulse pattern does not produce the receptor desensitization or side effect profile associated with direct GH injection.
A 2015 review in the Journal of Clinical Endocrinology confirming that GHRH analogs combined with ghrelin-pathway agonists produce a synergistic GH secretory response that exceeds additive effects when either compound is used alone provides the mechanistic basis for why combination therapy is the standard in supervised clinical settings.
What CJC-1295/Ipamorelin Does for Women: Six Benefits With a Timeline
The benefits of cjc 1295 ipamorelin for women correspond directly to the systems that decline when GH drops. This is not a general wellness intervention. Each effect maps to a specific physiological pathway that is disrupted by GH decline in the perimenopause transition.
Sleep Quality (Weeks 2 to 4)
GH secretion is highest during slow-wave, deep sleep. When GH declines, slow-wave sleep becomes lighter and less restorative, which compounds fatigue and reduces overnight recovery. CJC-1295/Ipamorelin amplifies the GH pulse that occurs during sleep without disrupting sleep architecture. Women consistently report this as the first noticeable effect, typically within 10 to 18 days of starting the protocol.
Body Composition and Fat Metabolism (Weeks 4 to 8)
GH activates lipolysis, particularly in visceral and subcutaneous fat. The perimenopause fat redistribution pattern, specifically the shift toward abdominal and flank storage, is partly a GH-decline phenomenon, not only an estrogen-decline phenomenon. Peptides for women weight loss that work through the GH axis address this redistribution specifically, not just total caloric balance. Measurable changes in body composition typically appear by weeks 6 to 8 in women who are combining the protocol with adequate protein intake and resistance training.
Skin Density and Hair Quality (Weeks 8 to 16)
IGF-1 drives collagen synthesis and fibroblast activity. As IGF-1 rises in response to increased GH, skin density improves and the hair cycle can normalize. Women who combine cjc 1295 ipamorelin for women with GHK-Cu peptide therapy at Perfect B often see more pronounced skin outcomes because both the GH-IGF-1 pathway and the collagen-stimulation pathway are being addressed simultaneously. The skin changes are not dramatic at 8 weeks but become clinically visible at the 12 to 16-week mark in most patients.
Muscle Preservation After 35
After 35, muscle loss accelerates in women partly because GH is a key signal for protein synthesis and lean tissue maintenance. CJC-1295/Ipamorelin is not an anabolic steroid. It does not build muscle the way testosterone does. What it does is preserve what exists and improve the body’s protein utilization response to resistance training. Women who start a supervised protocol during perimenopause maintain significantly more lean tissue through the transition than those who do not address the GH axis at all.
Energy and Cognitive Clarity
GH affects mitochondrial efficiency and neurotransmitter balance. Women on CJC-1295/Ipamorelin protocols consistently report improved daytime energy and a reduction in the cognitive fog that often appears during perimenopause. These effects are downstream of better sleep and improved metabolic function rather than a direct neurological effect of the peptide, which makes them durable rather than temporary.
Hormonal Feedback in Premenopausal Women
In women who are still cycling, improving the GH-IGF-1 axis can have downstream effects on the hypothalamic-pituitary-ovarian axis. This does not replace hormonal therapy when it is clinically indicated. It supports the hormonal environment more broadly and is a reason why the best peptides for women approaching perimenopause address multiple systems rather than a single deficiency.
Want to see what patients with your goals are running at Perfect B?
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
How CJC-1295/Ipamorelin Works Differently in Women Than in Men
The peptide molecules themselves do not change based on who receives them. The physiological environment they enter does. This distinction matters clinically because it determines dosing, timing, and what results to expect at each stage of the protocol.
Why Dosing Adjustment Is Not Optional
Women typically require lower doses than men because estrogen enhances GH receptor sensitivity. A woman who is still producing meaningful estrogen will have a stronger GH response per unit of peptide than a postmenopausal woman or a man at the same dose. At Perfect B in Doral, FL, cjc 1295 ipamorelin for women is dosed based on hormonal baseline labs, not body weight or a generic starting point. A woman in early perimenopause responds differently than one in full menopause, and the protocol reflects that difference from day one.
How the Menstrual Cycle Affects Response
Premenopausal women may notice variation in their response to cjc 1295 ipamorelin for women at different points in the cycle. GH secretion in women is higher in the follicular phase, when estrogen peaks, than in the luteal phase. This is not a problem with the protocol. It is a data point that, when tracked, helps calibrate dosing and timing with more precision than a static protocol ever could. Women working with Perfect B who are still cycling track this as part of their response monitoring.
A landmark clinical trial published in the Journal of Clinical Endocrinology and Metabolism demonstrating that Ipamorelin produces selective GH release without significant cortisol or prolactin elevation, establishing its safety profile for use in women with hormonally sensitive physiological backgrounds is the foundational study that shaped how the peptide is used today in supervised clinical settings.
What Results Look Like at 4, 8, and 12 Weeks for Women
The timeline for cjc 1295 ipamorelin for women follows a predictable pattern that most patients see, with variation based on starting hormonal status, sleep quality, diet, and training.
Weeks 1 to 4: Sleep Comes First
Deeper sleep is the dominant early change. Most women using peptides for women over 40 note that their sleep is more restorative by the end of the first month. Waking energy begins to stabilize. Some report a mild increase in vivid dreams during the first two weeks, which is a normal response to improved slow-wave sleep architecture and typically resolves on its own.
Weeks 4 to 8: Body Composition Begins Shifting
The scale may not change significantly in this window, but body composition does. Fat redistribution is measurable before it is visible. Women who track waist and hip measurements rather than weight alone capture this earlier. Muscle tone improves with resistance training because protein synthesis is more efficient. The real-patient outcomes documented in our CJC-1295/Ipamorelin before and after results from supervised patients at Perfect B reflect this pattern consistently across the patient population we treat in South Florida.
Weeks 8 to 12: The Full Clinical Picture
Skin texture, hair quality, and cognitive function show their most pronounced changes in this window. IGF-1 levels measured at the 12-week lab review typically confirm that the protocol is producing the expected physiological response. Most women at Perfect B continue beyond 12 weeks on a maintenance protocol, which is lower in frequency and sustains the gains made during the initial phase.
Who Is the Right Candidate for CJC-1295/Ipamorelin at Perfect B?
Not every woman searching for the best peptides for women over 40 is a candidate for CJC-1295/Ipamorelin at this time. The protocol requires clinical evaluation, baseline labs, and provider review before it begins.
Women Who Are Typically Strong Candidates
- Perimenopausal women (35 to 50) experiencing fatigue, sleep disruption, body composition changes, or cognitive fog that began after 35 and does not have another clear cause
- Postmenopausal women with low IGF-1 on baseline labs who have not started or are not candidates for traditional hormone replacement
- Premenopausal women with confirmed low IGF-1 and documented GH-axis symptoms who have ruled out thyroid dysfunction and other primary causes
- Women already on HRT who want to address the GH axis specifically, as CJC-1295/Ipamorelin and HRT work through separate mechanisms and are compatible under supervision
Who Should Not Start Without Specialist Evaluation
- Women who are pregnant or actively trying to conceive should not use CJC-1295/Ipamorelin without specialist reproductive endocrinology input
- Women with a history of hormone-sensitive cancers require oncology clearance before any GH-axis intervention
- Women with uncontrolled thyroid disease or active pituitary conditions need those issues addressed before starting peptide therapy
- Women with uncontrolled diabetes require careful monitoring because GH elevation affects insulin sensitivity
How CJC-1295/Ipamorelin Fits Into a Complete Protocol at Perfect B
At our clinic in Doral, FL, cjc 1295 ipamorelin for women is rarely prescribed as an isolated intervention. The patients who see the most complete results are those who address multiple systems simultaneously, because GH decline does not happen in isolation and neither does the recovery from it.
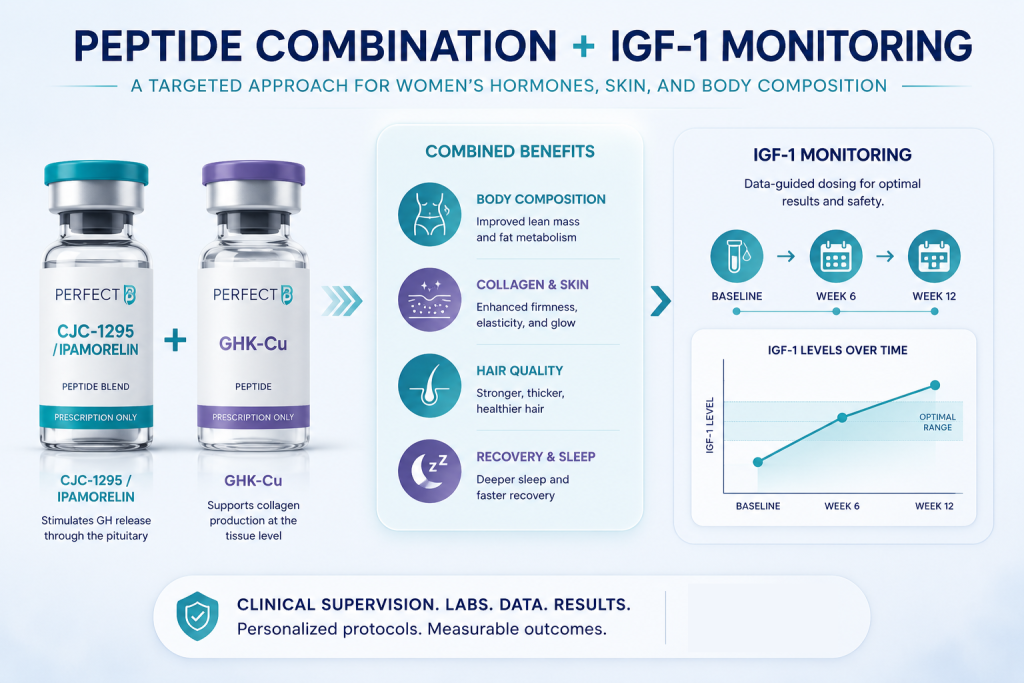
Combining With GHK-Cu for Skin and Hair
GHK-Cu operates through a different pathway than CJC-1295/Ipamorelin: it directly stimulates fibroblast activity and collagen gene expression at the tissue level. When both are active simultaneously, IGF-1 is rising from the GH-axis stimulation while local collagen synthesis is also being supported. Women targeting skin laxity and hair thinning see a more complete response from this combination than from either alone. The comprehensive approach to peptide therapy for women who want to address hormonal aging, body composition, and skin quality together is detailed in our peptide treatment plan at Perfect B, which outlines how we sequence and monitor each protocol for individual patient goals.
Why IGF-1 Monitoring Matters Throughout
IGF-1 is not just a marker of whether the protocol is working. Elevated IGF-1 beyond the optimal range is a signal to adjust the dose. At Perfect B, patients on cjc 1295 ipamorelin for women have IGF-1 measured at baseline, at 6 weeks, and at 12 weeks. This is the difference between a supervised protocol and buying peptides online: the data follows the patient, and the protocol follows the data.
What the Fat Loss and Menopause Connection Looks Like in Practice
Women who come to Perfect B looking for peptides for women weight loss through the GH axis often arrive after years of noticing that diet and exercise no longer produce the results they once did. The clinical explanation is not that willpower has failed. It is that the hormonal environment governing how fat is stored and mobilized has changed, and no amount of caloric restriction directly addresses GH pulse frequency.
CJC-1295/Ipamorelin does not replace the need for appropriate nutrition and training. What it does is restore the metabolic signaling environment that makes those inputs effective again. The fat redistribution pattern that defines perimenopause, specifically abdominal accumulation, responds to lipolytic GH signaling in a way that caloric restriction alone does not produce. For a broader look at how peptide therapy integrates with this clinical challenge, our post on peptides for fat loss during menopause and what the clinical evidence actually shows for women navigating midlife weight gain covers the full picture in detail.
Frequently Asked Questions
1. How long does it take to see results from CJC-1295/Ipamorelin as a woman?
Most women notice improved sleep quality within 2 to 3 weeks. Body composition changes typically become visible between weeks 4 and 8, depending on diet and training. Skin density and hair quality improvements are most pronounced at the 12 to 16-week mark. IGF-1 lab confirmation of a clinical response is measured at 6 and 12 weeks.
2. Do I need to cycle off CJC-1295/Ipamorelin, or can I take it continuously?
Cycling protocols vary based on clinical goals and individual response. Most supervised programs use an active phase of 12 to 24 weeks followed by a lower-frequency maintenance phase rather than a hard stop. The pituitary receptor system does not desensitize with CJC-1295/Ipamorelin at standard clinical doses the way it does with direct GHRH or older GHRPs, which is one of the reasons it became the preferred combination in supervised practice.
3. Is CJC-1295/Ipamorelin safe to use alongside hormone replacement therapy?
Yes, under clinical supervision. HRT addresses estrogen and progesterone. CJC-1295/Ipamorelin addresses the GH axis. These operate through different mechanisms and are not contraindicated together. In fact, women on estrogen replacement may see a stronger GH response to the peptide protocol because estrogen enhances pituitary GH sensitivity, which means dosing may need to be adjusted accordingly.
4. How is CJC-1295/Ipamorelin different from taking human growth hormone directly?
Direct HGH injection bypasses the pituitary entirely and suppresses the body’s own GH production over time. CJC-1295/Ipamorelin stimulates the pituitary to produce GH naturally, which preserves the pulse pattern and the feedback regulation that keeps IGF-1 in a safe range. The side effect profile of direct HGH (water retention, joint pain, insulin resistance at higher doses) is largely absent with CJC-1295/Ipamorelin at clinical doses because the physiological GH pulse is smaller and self-regulated.
5. What bloodwork do I need before starting at Perfect B?
A standard evaluation includes IGF-1, a complete metabolic panel, thyroid function, fasting glucose, and a hormonal panel appropriate for the patient’s cycle status. Depending on history, the provider may also request imaging or additional endocrine markers. No protocol begins at Perfect B without a complete baseline review.
6. Can CJC-1295/Ipamorelin help with perimenopause symptoms beyond body composition?
Yes. The GH axis contributes to sleep architecture, cognitive function, energy metabolism, skin integrity, and mood regulation, all of which shift during perimenopause. Women using peptides for perimenopause through the GH axis address a broader set of symptoms than those who focus only on estrogen supplementation. The two approaches are not mutually exclusive and many patients at Perfect B use both as part of a comprehensive perimenopause protocol.
Closing: The Clinical Bottom Line on CJC-1295/Ipamorelin for Women
CJC-1295/Ipamorelin for women is not a shortcut and it is not a supplement. It is a prescription peptide protocol that works precisely because it restores a specific physiological process that begins declining before most women realize it has started. The window between 35 and 45 is when this restoration is most effective, and the difference between a supervised clinical protocol and buying peptides online is not a matter of preference. It is a matter of safety, dosing accuracy, and IGF-1 monitoring that cannot be replicated without a provider and a lab.
At Perfect B in Doral, FL, CJC-1295/Ipamorelin is part of a clinical evaluation that begins with baseline labs, includes provider review of hormonal status, and is adjusted based on your response data throughout the protocol. The goal is not to override your physiology but to restore what it was doing at 30.
See what patients like you are running at Perfect B.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
- 📍 Visit us at Perfect B, Doral FL, serving Miami and South Florida patients seeking supervised growth hormone peptide therapy.
- 📞 Call (786) 502-2260 or message us today to schedule your CJC-1295/Ipamorelin consultation with a licensed medical provider.


