
Perfect B, Doral Fl. | 06.24.26 | 10 min read.
This article is for educational purposes only and does not constitute medical advice. Peptide therapy requires evaluation and prescription by a licensed medical provider. Do not use this information to self-administer or self-diagnose. Contact Perfect B at (786) 502-2260 to schedule a clinical evaluation.
What Peptides for Hormone Balance Actually Mean at Perfect B
Peptides for hormone balance is a phrase that arrives in our Doral, FL clinic with two opposing assumptions behind it. Some patients believe peptides can replace hormone therapy. Others assume any peptide will balance any hormone. Both are wrong, and the difference matters before a protocol is prescribed.
Peptides are short chains of amino acids that act as signaling molecules, telling specific cells to repair tissue, release growth hormone, support metabolism, or rebuild collagen. The peptides we prescribe at Perfect B do not replace estrogen, progesterone, or testosterone. They work on the growth hormone and IGF-1 axis. That axis sits upstream of body composition, sleep architecture, recovery, and tissue repair, and it is the lane peptides for hormone balance actually occupy in supervised clinical care.
This post explains which axis our peptides act on, which they do not, how peptides for hormone balance sit alongside hormone therapy when both are appropriate, and how Perfect B decides on a protocol from labs and InBody data rather than from a generic stack.

Not Sure Which Peptide Protocol Fits Your Hormone Picture? See What Patients With Similar Goals Are Running at Perfect B.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
Key Takeaways on Peptides for Hormone Balance
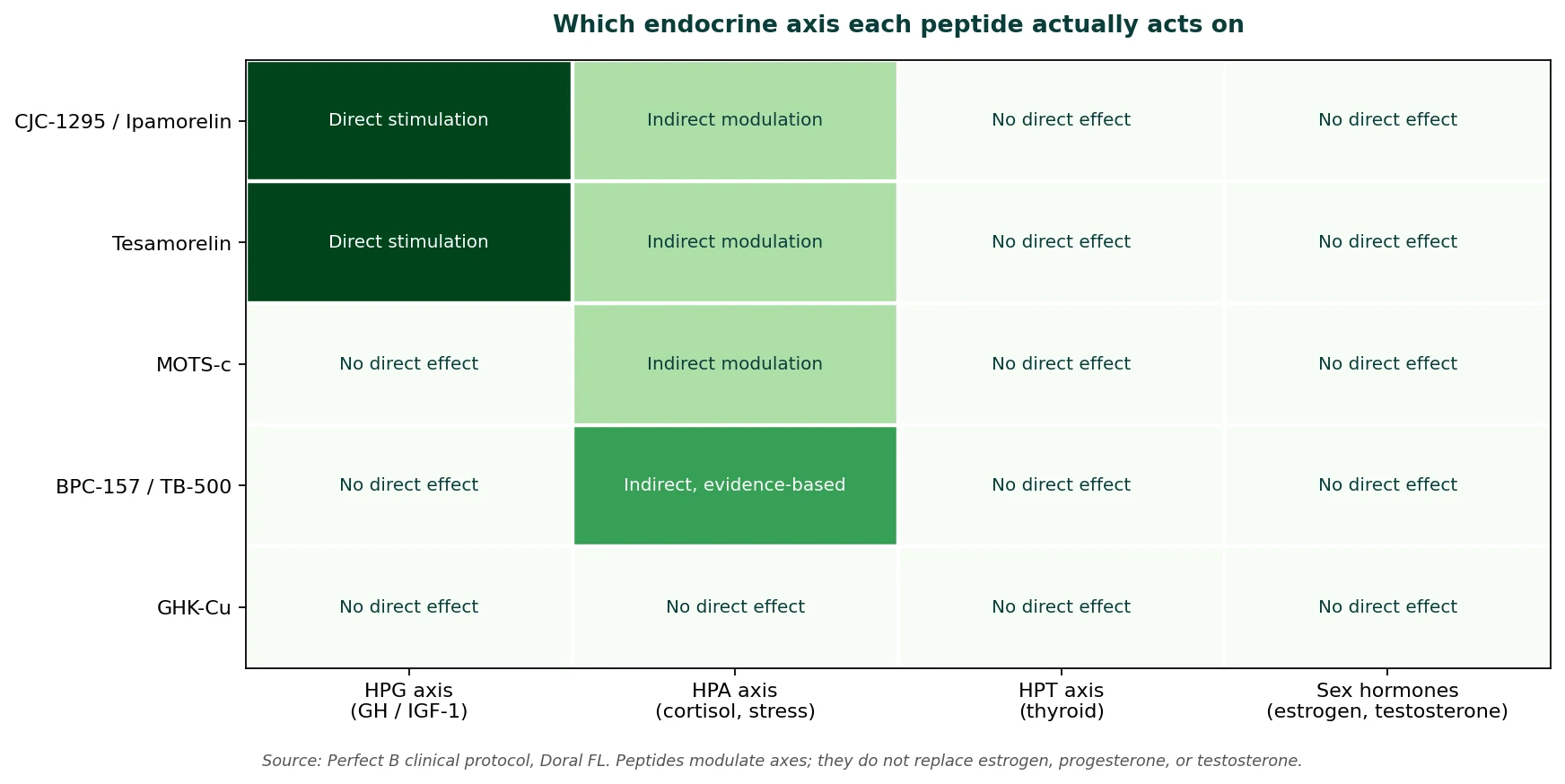
- Peptides are signals, not replacements: the peptides we prescribe at Perfect B act on the growth hormone and IGF-1 axis, not on sex hormones.
- Peptides do not replace hormone therapy: for patients in perimenopause, menopause, or with clinically low testosterone, peptides support sleep, body composition, and recovery alongside hormone therapy when appropriate, not instead of it.
- Two pathways exist, we use one: the growth hormone axis (CJC-1295, Ipamorelin, Tesamorelin) is what Perfect B prescribes. The gonadal axis (Kisspeptin, Gonadorelin, HCG) has narrower clinical use and is not in our standard menu.
- Lab work decides the protocol: estradiol, progesterone, testosterone, thyroid function, IGF-1, fasting glucose, HbA1c, lipid panel, plus an InBody scan, before anything is prescribed.
- Foundation first: nutrition, strength training, sleep, and hormonal evaluation come before any peptide decision. Peptides amplify a working system, they do not compensate for a broken one.
Why the Growth Hormone Axis Is Where Peptides for Hormone Balance Actually Work
Growth hormone is not a stable background signal. It pulses, primarily during deep sleep, and those pulses decline measurably starting at 35, a decade or more before menopause for women and before clinically low testosterone for men. When GH pulse frequency and amplitude drop, IGF-1 follows. Lower IGF-1 means reduced lean muscle preservation, slower collagen synthesis, impaired exercise recovery, and progressive changes to how the body partitions fat versus muscle. Patients describe lighter sleep, slower recovery, abdominal fat that did not exist before, and skin that has lost density. The pattern is consistent enough across our Doral, FL patient population that we screen for it directly with an IGF-1 lab and an InBody scan at the first visit.
Peptides like CJC-1295, Ipamorelin, and Tesamorelin act on this axis specifically. They signal the pituitary to release the patient’s own growth hormone in a pulsatile pattern that mirrors physiology, which is the mechanism we use when we talk about peptides for hormone balance. According to a 2021 peer-reviewed review documenting the role of peptide hormones discovered in the 21st century in the regulation of adipose tissue and metabolic function, this axis is where peptide-based intervention has the strongest mechanistic basis.
Two Pathways for Peptides and Hormones: What Perfect B Uses and What We Do Not
The phrase peptides and hormones gets used loosely online. Clinically there are two distinct pathways, and the difference defines what Perfect B can responsibly offer.
- The growth hormone axis (used at Perfect B): CJC-1295, Ipamorelin, and Tesamorelin act on the hypothalamic pituitary axis. They signal the pituitary to release the patient’s own growth hormone, which in turn drives IGF-1 production by the liver. Downstream effects include deeper sleep, faster recovery, improved insulin sensitivity, reduced visceral fat, and increased lean mass.
- The gonadal axis (not in our standard menu): Kisspeptin, Gonadorelin, and HCG act directly on the hypothalamic pituitary gonadal axis. They can raise testosterone directly because they trigger the testes to produce more of it. Perfect B does not include them in our standard peptide menu because the safety, dosing, and monitoring requirements are different from growth hormone axis peptides, and the use cases (fertility preservation during TRT, post-cycle therapy, hypothalamic dysfunction) are narrower than what most patients searching peptides for hormone balance actually need.

How Peptides for Hormone Balance Sit Alongside Hormone Therapy
This is the question we hear most often from patients comparing options. Peptides for hormone balance do not replace hormone therapy. For women in perimenopause and menopause, peptides support sleep, body composition, and recovery alongside hormone therapy when appropriate, not instead of it. For men whose total testosterone is well below range with broad symptoms, the honest clinical answer is TRT, sometimes with growth hormone axis peptides used alongside.
- Peptides alone: right when labs show declining IGF-1 but sex hormones are within range, and the symptoms cluster around sleep, recovery, body composition, and energy.
- Hormone therapy with peptides alongside: common after age 45. The hormonal foundation is addressed first or in parallel. Peptides for hormone balance amplify the recovery, sleep, and body composition response that hormone therapy alone does not fully restore.
- Hormone therapy alone: appropriate when labs confirm clear sex hormone deficiency and symptoms are dominated by what hormone therapy specifically addresses. Peptides will not substitute for that foundation.
Patients comparing their options often start by reading our clinical guide to peptides for women over 40 and what Perfect B actually prescribes in real protocols or our breakdown of peptides for testosterone and how they fit alongside TRT. Those posts cover the gender-specific clinical priorities. This post covers the axis logic that sits behind both.
See How Perfect B Decides Which Peptide Fits Your Hormone Picture.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
What About Peptides for Thyroid and Peptides for Cortisol?
These are two common searches that arrive together with peptides for hormone balance, and the honest answer is the same for both.
The peptides we prescribe at Perfect B do not act on the thyroid directly. We screen the thyroid panel as part of the baseline labs because thyroid dysfunction can blunt peptide response, and an abnormal result is flagged for the patient and their primary care provider. Peptides for thyroid as a category of direct treatment are not part of our menu, and we will tell patients that on the first call instead of selling something that does not exist.
The same applies to peptides for cortisol. None of the peptides in our protocol directly suppresses or stimulates cortisol. What restoring the growth hormone axis does is improve sleep architecture, and better sleep is the single most reliable lever on chronic cortisol load. The effect is indirect and works through sleep, not through the adrenal axis itself.
The Perfect B Peptide Catalog Behind Hormone Balance, by Goal
Peptides for hormone balance is not a single product. The right choice depends on what each patient is trying to change. Every peptide we prescribe at Perfect B falls into one of the categories below, and we do not prescribe Sermorelin, PT-141, Kisspeptin, Gonadorelin, Selank, DSIP, Thymosin Alpha-1, or research-grade peptides sold online.
- CJC-1295 with Ipamorelin: the most requested growth hormone peptide stack at our Doral clinic. CJC-1295 is a GHRH analog with an extended half-life. Ipamorelin binds the ghrelin receptor in the pituitary through a separate pathway. Together they produce a synergistic GH pulse that neither achieves alone. Used for sleep, body composition, recovery, and energy.
- Tesamorelin: a GHRH analog that is FDA-approved for visceral fat reduction in HIV-associated lipodystrophy and used clinically for non-HIV visceral fat in supervised settings. We use it when an InBody scan shows visceral fat above 10 and the patient’s broader picture supports it.
- GHK-Cu: a copper peptide with one of the strongest research records in skin biology. Used when skin density, collagen, and visible aging are the primary concerns. Pairs naturally with in-clinic skin treatments rather than competing with them.
- BPC-157 with TB-500 (the Wolverine stack): tissue repair peptides used for recovery, joint discomfort, tendon strain, and gut integrity. Not a hormone peptide. Listed here because it commonly stacks with growth hormone axis peptides when recovery is part of the hormone balance picture.
- MOTS-c: a mitochondrial peptide studied for cellular energy production, insulin sensitivity, and long-term body composition. Useful when fatigue and metabolic stalling sit alongside the hormonal picture.
Notice what is not on this list. No peptide in our protocol replaces estrogen, progesterone, or testosterone. For the broader endocrine framework that sits behind hormone therapy decisions, the Endocrine Society patient resource on hormones and endocrine function is a clean reference for the system peptides for hormone balance work alongside.
The Foundation Before Peptides for Hormone Balance
Peptides do not work in a vacuum. They amplify a system that is already functioning. At Perfect B in Doral, the prerequisites before any peptide decision are not optional, and skipping them is the most common reason patients see disappointing results and conclude the molecules do not work.
- Baseline labs: a comprehensive hormonal and metabolic panel including estradiol, progesterone, testosterone, thyroid function, IGF-1, fasting glucose, HbA1c, and lipid panel. These tell us where the hormonal axis currently sits and what is influencing it.
- InBody body composition scan: visceral fat, skeletal muscle mass, and segmental composition before any peptide is prescribed. Visceral fat above 10 changes the protocol toward Tesamorelin. Low skeletal muscle mass with normal visceral fat points to CJC-1295 with Ipamorelin.
- Hormonal evaluation when relevant: if a patient is in perimenopause, menopause, or has clinically low testosterone, the question of whether hormone therapy is needed is addressed first or alongside the peptide decision. Peptides for hormone balance are not a substitute for hormone therapy when hormone therapy is indicated.
- Nutrition and strength training: protein adequacy and consistent resistance training are central, not optional. Lean mass preservation is the single most important variable for body composition outcomes after 35, and no peptide will compensate for an absence of strength training.
- Sleep: growth hormone peptides work primarily during deep sleep. A patient sleeping four broken hours a night will see less response than one sleeping seven consistent hours.
What Patients Notice First on Peptides for Hormone Balance
The axis is the same in both sexes. What differs is which symptom shifts first, because the baseline complaint is different.
- Women in perimenopause and menopause: deeper, more restorative sleep within 2 to 3 weeks of starting a CJC-1295 with Ipamorelin protocol. Body composition changes typically follow over the next 2 to 3 months as the growth hormone pulse normalizes.
- Men in their 40s and 50s with visceral fat and slower recovery: energy and morning alertness shift first, usually by week 3 to 4. Body composition changes follow by week 8 to 12.
- Both: recovery from training improves earliest, sometimes by the end of week 2. This is the most consistent signal across the patients we see at our Doral clinic.

Frequently Asked Questions About Peptides for Hormone Balance
1. Do peptides affect hormones the same way hormone therapy does?
No. Peptides for hormone balance act on signaling pathways, mostly the growth hormone and IGF-1 axis. Hormone therapy directly replaces a deficient hormone such as estrogen, progesterone, or testosterone. Peptides and hormones cooperate in supervised care but are not interchangeable.
2. Can peptides for hormone balance replace my estrogen, progesterone, or testosterone prescription?
No. Peptides we prescribe at Perfect B address a different layer of the system. If you need hormone therapy, peptides for hormone balance can sit alongside it but do not replace it.
3. Are there peptides for cortisol and stress?
Not directly. No peptide in our Perfect B protocol suppresses or stimulates cortisol on its own. What peptides for hormone balance do is restore the growth hormone pulse during deep sleep, and better sleep is the single most reliable lever on chronic cortisol load.
4. Are there peptides for thyroid at Perfect B?
Not as a category of direct thyroid treatment. We screen the thyroid panel as part of baseline labs because thyroid dysfunction can blunt peptide response, but the peptides themselves act on the growth hormone axis, not on the thyroid.
5. How long before peptides for hormone balance start working?
Patients in our Doral, FL clinic typically notice sleep and recovery changes within 2 to 4 weeks of starting a CJC-1295 with Ipamorelin protocol. Body composition changes show on InBody by week 8 to 12.
6. What labs do you need before starting a peptide protocol at Perfect B?
Estradiol, progesterone, testosterone, thyroid function, IGF-1, fasting glucose, HbA1c, and lipid panel, plus an InBody body composition scan. The labs decide which peptides for hormone balance fit your physiology.
7. Do peptides for hormone balance work the same in men and women?
The growth hormone axis is the same in both sexes, but the clinical priorities differ. Women in perimenopause often need hormone therapy alongside peptides. Men with clinically low testosterone often need TRT alongside peptides. The peptide protocol itself can be similar.
Closing: The Clinical Bottom Line on Peptides for Hormone Balance
Peptides for hormone balance are powerful when they are matched to the right axis, the right lab profile, and the right patient. They are not a replacement for hormone therapy, they are not a fix for thyroid disease, and they are not a shortcut around poor sleep or untreated insulin resistance. They are a precise tool that restores growth hormone and IGF-1 signaling in adults whose own axis has declined.
The difference between a supervised peptide protocol at a medical clinic in Doral, FL and a grey-market vial ordered online is everything that sits behind the injection: the labs, the protocol logic, the contraindication screening, and the follow-up. If you want the protocol matched to your physiology rather than to a marketing claim, that is what the consultation is for.
- 📍 Visit us at Perfect B | 3905 NW 107th Ave, Suite 104, Doral FL 33178
- 📞 Call or message us at (786) 502-2260
- 💳 Buy Now Pay Later available: Cherry, Klarna, Afterpay, CareCredit
→ Book your peptide consultation at Perfect B in Doral today.


