
Perfect B, Doral Fl. | 05.18.26 | 13 min read.
This article is for educational purposes and does not replace a medical evaluation. Treatments mentioned require a personalized consultation with a licensed medical provider in Florida. Information based on peer-reviewed dermatology literature and clinical experience at our Doral medical aesthetic clinic.
Acne can heal and leave behind a different problem: flat pink, red, or purple marks that linger long after the pimple is gone. These marks are not scars. They are not melanin spots either. They are a vascular condition called post-inflammatory erythema, or PIE, and the way you treat them depends entirely on understanding what they actually are.
This guide explains what PIE is, how it differs from its dark-mark cousin PIH, what works at home, what works in-office, and why Miami’s heat and humidity make PIE a stubborn problem for many South Florida patients. Everything here reflects peer-reviewed dermatology evidence and the clinical protocols we use daily at our Doral practice.
Key Takeaways on Post-Inflammatory Erythema (PIE)
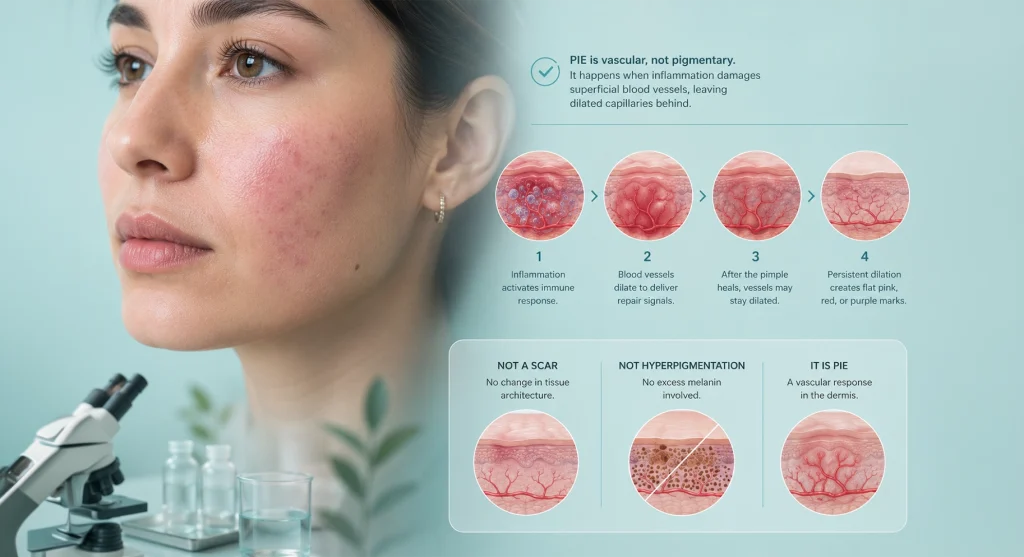
- PIE is vascular, not pigmentary. It is caused by dilated or damaged capillaries near the skin surface, not by melanin overproduction. That distinction changes everything about treatment.
- Most cases fade in 3 to 6 months. Roughly 20 percent of cases persist for years without professional intervention, especially in patients with severe cystic acne history or chronic sun exposure.
- The blanch test is the diagnostic anyone can run. Press a clear glass on the mark. If the color briefly disappears (blanches), it is PIE. If the color stays the same, it is PIH.
- Topical niacinamide 5 percent, azelaic acid, vitamin C, and retinoids have clinical evidence supporting PIE management. Each works through a different mechanism.
- Pulsed dye laser (PDL) is the in-office gold standard, with IPL and KTP laser as effective alternatives. About 95 percent of dermatologists consider PDL first-line therapy for persistent PIE.
What Is Post-Inflammatory Erythema and Why Does It Happen?
Post-inflammatory erythema is the formal medical term for the flat pink, red, or purple discoloration that remains after an inflammatory acne lesion heals. The term was coined in 2013 by Bae-Harboe and Graber at Boston University Department of Dermatology, who published their findings in the Journal of Clinical and Aesthetic Dermatology. Before that paper, there was no standard term to separate these vascular marks from dark melanin marks (PIH), and treatment outcomes suffered because of the confusion. You can read the foundational paper, Easy as PIE (Postinflammatory Erythema) by Bae-Harboe and Graber published in the Journal of Clinical and Aesthetic Dermatology in 2013, on the National Library of Medicine PubMed Central archive.
Here is the actual mechanism. When you develop an inflammatory pimple (a papule, pustule, or cyst), your immune system rushes white blood cells, signaling molecules, and inflammatory cytokines to the site. Blood vessels near the surface dilate to deliver these repair components. Once the inflammation resolves and the pimple heals, those tiny capillaries are supposed to constrict back to baseline. Sometimes they do not. They stay dilated, or the inflammation damaged the vessel walls in a way that leaves them visibly stretched. The result is a flat mark in pink, red, or purple, depending on your skin tone and how deep the vessels sit.
This is not a scar. Scars involve tissue architecture change, either depressed (atrophic) or raised (hypertrophic). PIE is the dermis-level vascular footprint of inflammation that has otherwise fully healed at the skin surface. This is also not hyperpigmentation. There is no excess melanin involved.
PIE vs PIH: The Blanch Test and the 4 Other Ways to Tell Them Apart
The single most useful at-home test for distinguishing PIE from post-inflammatory hyperpigmentation (PIH) is the blanch test. Here is how to do it.
- Find a clean, clear glass slide or the bottom of a clear drinking glass.
- Press it firmly against the mark for about 5 seconds while looking through the glass.
- Watch what happens to the color directly underneath the pressure point.
If the mark briefly turns white (blanches) and then returns to its original color when you release pressure, you are dealing with PIE. The pressure temporarily emptied the dilated capillaries, which is only possible if the color comes from blood. If the mark stays the same color under pressure, you are dealing with PIH. Melanin pigment does not move when compressed, so the color persists.

Beyond the blanch test, here are 4 additional clinical differences that determine treatment strategy:
- Color: PIE appears pink, red, or purple. PIH appears brown, gray, or sometimes black. The redder the mark, the more likely PIE. The darker and warmer the mark, the more likely PIH.
- Mechanism: PIE is vascular (blood vessels). PIH is pigmentary (melanin). One is a blood vessel issue, the other is a pigment-producing cell (melanocyte) issue.
- Fitzpatrick skin type pattern: PIE is more common and visible in Fitzpatrick types I through III (lighter skin), though it also occurs in types IV through VI where it appears violet or dark purple. PIH is far more common in types IV through VI.
- Treatment gold standard: PIE responds to vascular treatments (pulsed dye laser, IPL, KTP laser). PIH responds to melanin inhibitors, chemical peels, and skin cell turnover accelerators like retinoids.
An important reality: PIE and PIH can coexist in the same patient and even within the same individual lesion, especially in Fitzpatrick III through V skin (common in Miami’s Hispanic and Caribbean population). If you have both, your treatment plan needs to address both pathologies. For a detailed walkthrough of the dark-mark side of this equation, see our companion guide, Post-Inflammatory Hyperpigmentation (PIH): Dark Marks, Red Spots, and What a Miami Clinic Actually Uses, which covers the pigmentary half of post-acne discoloration in detail.
What Causes PIE: Inflammation, Picking, and the Capillary Damage Cascade
Five factors drive PIE formation, alone or in combination:
- Inflammatory acne lesions. Papules, pustules, nodules, and cysts trigger the deepest immune response. The bigger and deeper the pimple, the more likely it leaves PIE behind. Closed comedones and blackheads rarely cause PIE because the inflammation is minimal.
- Picking, squeezing, or popping. This is the biggest accelerator of PIE we see at our clinic. Mechanical trauma compounds the inflammatory damage, pushes contents into surrounding tissue, and extends both healing time and capillary damage.
- Aggressive skincare or over-exfoliation. Using too many actives at once, scrubbing too hard, or stripping the skin barrier creates chronic low-grade inflammation that primes capillaries to stay dilated.
- Sun exposure during healing. UV radiation prolongs inflammation, slows capillary repair, and can convert what would have been transient PIE into long-lasting PIE.
- Heat exposure and chronic flushing. Hot showers, saunas, intense workouts, and tropical climates temporarily dilate facial capillaries. Repeated dilation in already-damaged vessels makes PIE more visible and slower to fade.
How Long Does PIE Take to Fade? The 3 to 6 Month Window and the 20 Percent That Does Not

For most patients, PIE fades on its own within 3 to 6 months once the underlying acne is controlled. The body slowly remodels damaged capillaries, the inflammation fully resolves, and skin color returns to baseline. This is the typical timeline that most dermatology sources cite, and it holds for the majority of cases involving mild to moderate inflammatory acne.
But here is the part most online guides skip: roughly 20 percent of PIE cases do not resolve naturally. They persist for 12 months or longer, sometimes indefinitely, without professional intervention. We see this pattern in patients who fit one or more of these profiles:
- History of severe cystic or nodular acne with multiple deep lesions in the same area
- Years of picking or squeezing pimples before seeking care
- Chronic sun exposure without consistent SPF use (very common in South Florida)
- Compromised skin barrier from over-treatment with harsh products
- Mature patients (over 40), where capillary repair capacity is naturally slower
The practical takeaway: if your PIE has not visibly improved after 4 to 6 months of consistent home care, the natural-fade window is closing and professional vascular treatment becomes the realistic path forward. Waiting indefinitely rarely helps once you are past that window, because the capillary damage has stabilized.
PIE in Fitzpatrick III to V Skin: When Red Looks Violet or Purple
The standard textbook teaching is that PIE primarily affects Fitzpatrick I through III (lighter skin), while PIH primarily affects Fitzpatrick IV through VI (medium to darker skin). That rule is broadly true, but it can mislead patients who have a mix of skin tones (the majority of our Doral patient population).
In Fitzpatrick III through V skin, common in Hispanic, Caribbean, and Mediterranean populations, PIE often presents differently than the classic pink or red appearance:
- Marks may look violet, dusky pink, or dark plum rather than bright red
- The blanch test still works (vascular marks blanch regardless of skin tone), but the color shift may be subtle and harder to see
- PIE frequently coexists with PIH in the same lesion, creating a layered red and brown appearance
- Both pathologies require concurrent treatment, not sequential
When we evaluate PIE in patients with deeper skin tones at our Doral clinic, we adjust the protocol in three ways. First, laser test spots are mandatory before full-area treatment to verify melanin response and prevent post-laser hyperpigmentation. Second, we typically use lower fluence settings and longer wavelengths (for example, longer-pulse PDL or 1064 nm vascular lasers). Third, we layer topical melanin inhibitors and strict photoprotection alongside the vascular work to prevent the PIH side of the equation from worsening during laser sessions.
Daily Skincare for PIE: The Ingredients With Clinical Evidence

Four topical ingredients have clinical evidence supporting their use in PIE management. None of them will erase PIE overnight, but consistent daily use over 8 to 12 weeks accelerates fading and can prevent new PIE from forming if you still have active acne.
1. Niacinamide 5 Percent (Topical Vitamin B3)
Niacinamide at 5 percent is the strongest evidence-backed topical for redness reduction. A 12-week double-blind, placebo-controlled split-face study by Bissett and colleagues (published in 2005) demonstrated that 5 percent niacinamide significantly reduced red blotchiness, hyperpigmentation spots, and texture irregularities compared to placebo. The mechanism: niacinamide inhibits the inflammatory cytokine IL-8 through the NF-kB pathway, supports the skin barrier, and modulates the inflammatory cascade that keeps PIE capillaries dilated. Apply morning and night under moisturizer. For a deeper look at this ingredient, see Niacinamide Benefits: What This Ingredient Actually Does for Your Skin, our full guide on niacinamide.
2. Azelaic Acid 10 to 20 Percent
Azelaic acid is anti-inflammatory and mildly brightening. It is one of the few ingredients that targets both PIE (through inflammation reduction) and PIH (through melanin inhibition), making it particularly useful for mixed cases common in our Doral patient population. It is also exceptionally well tolerated, including by pregnant patients (with provider guidance) and sensitive skin types. Apply once nightly, building up to twice daily if tolerated.
3. Vitamin C (L-Ascorbic Acid 10 to 20 Percent)
Vitamin C strengthens capillary walls, neutralizes UV-induced free radicals, and supports collagen synthesis. For PIE specifically, the capillary-wall benefit matters because stronger vessels are less likely to stay dilated after inflammatory insult. Use a stable L-ascorbic acid formulation at 10 to 20 percent or a more tolerable ester form like sodium ascorbyl phosphate. Apply in the morning, under your sunscreen. Vitamin C and SPF together are also the best photoprotection combination available.
4. Topical Retinoids (Tretinoin, Adapalene)
Retinoids improve dermal remodeling, accelerate cell turnover, and (most importantly for PIE prevention) control the inflammatory acne that creates new PIE in the first place. They are not a fast fix for existing PIE, but they prevent the next round. Start at low frequency (2 to 3 nights per week) and build up over 6 weeks. Apply at night only, always pair with morning SPF, and expect 4 to 6 weeks of skin adjustment.
What Makes PIE Worse in Miami’s Climate: Heat, Humidity, and UV
South Florida’s climate creates four PIE-aggravating conditions that patients from cooler climates do not have to manage. Most online PIE guides ignore this entirely, which is why our patients often see better results once we adjust their routine to local conditions.
- Sustained heat above 86°F (30°C). Miami averages this temperature roughly 6 to 8 months a year. Heat causes peripheral vasodilation, including in facial capillaries. Repeated dilation in already-damaged vessels makes PIE flare daily and slows the natural fade cycle.
- Humidity above 70 percent. Tropical humidity disrupts the skin barrier by altering transepidermal water loss patterns and increasing bacterial load on the skin. A compromised barrier means more low-grade inflammation, which sustains PIE.
- UV index of 9 to 11 most of the year. Doral and the greater Miami area sit at a latitude where UV exposure peaks at “very high” or “extreme” on the index from March through October. UV worsens both PIE (through inflammation) and PIH (through melanin stimulation) simultaneously.
- Indoor/outdoor temperature cycling. Going repeatedly between strong air conditioning and humid outdoor heat causes vascular reactivity in the face, which manifests as visible flushing and aggravates baseline PIE.
The practical adjustments we recommend to our Doral patients: wash your face with lukewarm water, never hot. Limit hot showers and skip facial saunas. Use broad-spectrum mineral or hybrid SPF 50 or higher every morning and reapply every two hours when outdoors. Stay in air conditioning during peak heat hours (11 AM to 3 PM) if possible. Skip alcohol-based toners that strip the barrier in humid conditions, and choose hydrating, ceramide-rich moisturizers instead.
In-Office Treatments for PIE: PDL, IPL, and KTP Laser at Our Doral Clinic
When topicals alone are not enough, three in-office vascular treatments at Perfect B Doral address PIE directly.
Pulsed Dye Laser (PDL)
Pulsed dye laser is the consensus first-line therapy for PIE. Approximately 95 percent of dermatologists rank it as the gold standard for residual acne erythema, and clinical studies have shown up to 82 percent reduction in PIE lesion appearance after a single treatment, with optimal results visible around 12 weeks post-procedure. PDL works by emitting a wavelength (typically 585 to 595 nm) that is selectively absorbed by oxyhemoglobin in the dilated capillaries. The vessels heat up, coagulate, and the body clears them over the following weeks. Most patients require 1 to 3 sessions spaced 4 to 6 weeks apart. Downtime is minimal: mild redness or temporary purpura (bruising) for a few days, depending on settings.
IPL (Intense Pulsed Light)
IPL uses a broad spectrum of light (typically 500 to 1200 nm with filters) to target hemoglobin in vascular lesions. A clinical study by Mathew and colleagues published in the Indian Dermatology Online Journal in 2018 confirmed IPL’s efficacy specifically for acne-induced post-inflammatory erythema. IPL is a strong option when PIE is diffuse across larger facial areas (cheeks, jawline, forehead) rather than concentrated in a few spots, and when the patient also has generalized facial redness or sun-induced telangiectasias. We typically program 3 to 5 sessions, 4 weeks apart.
KTP Laser (Potassium Titanyl Phosphate, 532 nm)
KTP laser at 532 nm is highly absorbed by oxyhemoglobin and is excellent for fine surface telangiectasias and discrete PIE lesions that have not fully responded to PDL or IPL. We use KTP as a complementary modality, often alternating with PDL across the treatment plan or as a touch-up for stubborn individual spots. It is also a good option for patients in Fitzpatrick III to V skin where shorter wavelengths require careful melanin management.
When We Add Chemical Peels, LED Therapy, or Microneedling
Chemical peels (salicylic, glycolic, mandelic, lactic, TCA) at appropriate depths help when PIE coexists with surface texture changes or mild PIH. LED therapy (especially yellow and red light) is a useful anti-inflammatory adjunct between laser sessions. Microneedling with PRP and RF microneedling (Morpheus8) come into the conversation only when PIE coexists with atrophic acne scars; these treatments address texture, not vascular pathology directly. For a full picture of how we sequence treatments when PIE, PIH, and scarring coexist, see Acne Scar Treatment in Miami: How Perfect B Treats Every Scar Type with a Staged Medical Plan, our staged acne scar treatment plan for South Florida patients.
For a complete view of our combination protocol for patients with both vascular and textural acne sequelae, see our Acne Scars Treatment Plan, which outlines how PDL, peels, microneedling, and other modalities are staged across a 6 to 12 month protocol.
The Build-Up Protocol: 6-Week Daily Routine for South Florida Patients
This is the introductory routine we hand to most PIE patients at our Doral clinic. It is paced for skin barrier safety (no shock from too many actives at once) and adapted for Miami’s heat and UV reality.
Weeks 1 to 2: Foundation and Barrier
- AM: Gentle non-foaming cleanser with lukewarm water, hyaluronic acid serum, ceramide moisturizer, broad-spectrum SPF 50 or higher
- PM: Same cleanser, moisturizer, no actives yet
- Goal: rebuild barrier, eliminate hot water and harsh exfoliants, lock in SPF habit
Weeks 3 to 4: Add Niacinamide and Vitamin C
- AM: Cleanse, vitamin C serum 10 to 20 percent, niacinamide 5 percent serum, moisturizer, SPF 50+
- PM: Cleanse, niacinamide 5 percent serum, moisturizer
- Goal: establish redness-reduction baseline, get used to actives without irritation
Weeks 5 to 6: Add Azelaic Acid and Begin Retinoid
- AM: Cleanse, vitamin C, niacinamide, moisturizer, SPF 50+
- PM: Cleanse, azelaic acid 10 percent (alternating nights with retinoid), low-dose retinoid 2 to 3 nights per week, moisturizer
- Goal: full active stack, prevent new PIE, support fade of existing marks
Week 7 Forward: Evaluate and Decide on In-Office Care
- Continue full routine
- Photograph PIE areas weekly under consistent lighting
- If visible fading by week 10 to 12, continue and reassess at month 6
- If no visible fading by week 10 to 12 or PIE is over 6 months old already, schedule an in-office consultation for vascular laser evaluation
When to Stop Waiting and See a Medical Provider
PIE is medically harmless, so there is no urgent health timeline. But there is a quality-of-life and treatment-feasibility timeline that matters. Schedule a consultation if any of the following apply:
- Your PIE has not visibly improved after 4 to 6 months of consistent home care with proven actives and SPF discipline
- The marks are affecting your confidence, social comfort, or makeup routine in a way you no longer want to manage
- You have active acne alongside the PIE, which means new lesions are continuing to create new PIE faster than the old marks fade
- You have a mix of PIE plus PIH plus textural scarring, which requires a coordinated treatment plan rather than ad-hoc topicals
- You are Fitzpatrick IV, V, or VI and want a protocol designed for melanin protection alongside vascular treatment
- You are preparing for a major event (wedding, photo session, milestone) within the next 6 to 12 months and want to optimize results
At our Doral medical aesthetic clinic, every PIE consultation begins with a full skin evaluation under standardized lighting, a personal acne and skincare history, identification of Fitzpatrick type and PIE vs PIH coexistence, photo documentation, and a written staged plan that balances home care, in-office vascular treatment, and prevention. You can reach us at +1 (786) 502-2260 to schedule.
Frequently Asked Questions About Post-Inflammatory Erythema
1. Is PIE the same as an acne scar?
No. PIE is flat discoloration from dilated capillaries with no underlying tissue change. True acne scars (ice pick, boxcar, rolling, atrophic, hypertrophic) involve structural damage to the dermis that affects skin texture. PIE can fade fully on its own; structural acne scars usually cannot.
2. Can PIE fade on its own without any treatment?
For most patients, yes. Approximately 80 percent of PIE cases fade naturally within 3 to 6 months once the underlying acne is controlled and skin is protected from sun and irritation. The 20 percent that do not fade within 12 months typically require in-office vascular treatment to fully resolve.
3. Does daily sunscreen really matter for PIE?
Yes, more than for almost any other post-acne issue. UV exposure prolongs the inflammatory response that keeps capillaries dilated, slows vascular repair, and can convert temporary PIE into long-term PIE. In Miami’s climate (UV index 9 to 11 most of the year), daily broad-spectrum SPF 50 or higher with reapplication is non-negotiable for PIE recovery.
4. Can I use niacinamide, vitamin C, azelaic acid, and a retinoid all at once?
Yes, but not on day one. The build-up matters. Start with niacinamide and vitamin C for 2 to 4 weeks, then add azelaic acid, then add a retinoid at low frequency. Splitting AM (vitamin C, niacinamide) and PM (azelaic acid, retinoid) reduces interaction concerns and irritation risk. If your skin is sensitive or your barrier is already compromised, your provider may sequence this differently.
5. How is PIE diagnosed at Perfect B Doral?
We diagnose PIE through clinical examination under standardized lighting, the blanch test for vascular confirmation, dermatoscopy when needed, and a structured patient history (acne severity timeline, picking habits, sun exposure, prior treatments, Fitzpatrick assessment). PIE diagnosis is clinical (no biopsy needed) and usually unambiguous once you know the signs to look for.
6. What is the difference between PIE and rosacea redness?
PIE is localized, flat, and traces directly back to specific resolved inflammatory lesions (acne, picking, irritation). Rosacea redness is diffuse, often triggered by flushing (heat, alcohol, spicy food, stress), and frequently involves visible broken capillaries (telangiectasias), papules, and a chronic background flush. The two can coexist, and patients with both need a combined treatment plan that addresses each pathology distinctly.
7. Can heat or exercise make my PIE worse permanently?
Temporarily, yes. Permanently, no, but the temporary flare effect can be frequent enough that it feels permanent. Heat dilates facial capillaries, which makes PIE more visible during and after the heat exposure. The capillaries return to baseline within 30 to 90 minutes. If your PIE is severe or affecting confidence, it is reasonable to modify post-workout cooldowns, avoid saunas, and use lukewarm showers as part of your routine.
8. Why does my PIE look violet or purple instead of red?
Skin tone changes how PIE appears. In Fitzpatrick III through V (common in Latino, Caribbean, and Mediterranean patients), the underlying melanin makes dilated capillaries appear violet, dusky pink, or dark plum rather than the bright red typical in Fitzpatrick I or II skin. The condition is the same vascular pathology. The blanch test still confirms the diagnosis.
Why Acting on PIE Early Matters in Miami’s Climate
PIE is medically harmless, but it is also one of the most under-treated post-acne issues we see at our Doral clinic. Patients commonly assume the red marks are scars (they are not), or wait 18 months hoping nature will resolve what is actually persistent vascular damage. Meanwhile, daily heat exposure, UV, and any continued acne keep recreating the same problem.
The earlier you intervene with the right diagnosis, the right topicals, and (if needed) the right vascular laser protocol, the shorter your recovery window becomes and the less risk you carry of permanent vascular damage. In a climate like ours, where the underlying conditions for PIE worsen seasonally, that distinction can be the difference between months of stalled progress and a clear, predictable timeline to resolution.
📍 Perfect B Medical Aesthetic Clinic, Doral, FL
📞 +1 (786) 502-2260


