
Perfect B, Doral Fl. | 06.23.26 | 11 min read.
This article is for educational purposes only and does not constitute medical advice. Peptide therapy requires evaluation and prescription by a licensed medical provider. Do not use this information to self-administer or self-diagnose. Contact Perfect B at (786) 502-2260 to schedule a clinical evaluation.
What “Best Peptides for Women Over 50” Actually Means
There is no single best peptide for women over 50. The right choice depends on what a patient is trying to change. Most articles answer this query with a generic stack of five or six peptides as if biology after 50 were a checklist. It is not. After menopause is complete, the priorities shift away from optimizing perimenopause and toward preserving lean mass, protecting bone density, supporting longevity biomarkers, restoring skin architecture, and improving recovery. At Perfect B in Doral, FL we organize the catalog by clinical goal and validate the choice with an InBody scan and baseline labs before anyone touches a vial.
This is the post-menopausal version of the conversation, not the perimenopause one. For women in their 40s who are still cycling or just entering perimenopause, the peptide answer is different. We cover that pattern in our clinical guide to peptides for women over 40 and how the perimenopausal protocol differs from the post-menopausal one.

Not Sure Which Peptide Fits Your Profile After 50? See What Women Patients Over 50 Are Running at Perfect B.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
Key Takeaways
- The catalog is chosen by goal, not by age alone. Skin, sleep, body composition, recovery, visceral fat, and longevity each have a different peptide answer.
- The biology at 50 is not the biology at 40. Estrogen decline is consolidated, the growth hormone axis has dropped further, and sarcopenia plus bone density loss become primary risks rather than emerging ones.
- Foundation first. Hormone status, nutrition, resistance training, and sleep have to be in place. Peptides amplify a working system. They do not replace it.
- Peptides complement hormone therapy, they do not replace it. Women already on hormone replacement therapy can layer peptides for goals HRT does not address.
- Supervision is the product. Self-sourced peptides from online sellers do not have the same active compound, sterility, or dosing accuracy as compounded prescriptions from a medical clinic.
Why the Biology at 50 Is Different From the Biology at 40
Growth hormone production starts declining at 35, not at menopause. By the time a woman reaches her early fifties, the decline has been compounding for fifteen years on top of the estrogen drop that defines the menopausal transition itself. The result is a different physiology, not just an older version of the same one.
Four changes drive the protocol after menopause. Bone density loss accelerates in the first five to seven years post-menopause, which is the highest-risk window for accelerated osteoporosis and the reason DEXA scans become routine after 50. Sarcopenia, the age-related loss of skeletal muscle, accelerates roughly one percent per year if nothing intervenes. Collagen synthesis drops sharply, which shows up first in skin atrophy and slower wound healing. Sleep architecture fragments, with deep sleep specifically becoming harder to reach, which slows the recovery the muscle and skin need.
What Changes Compared to the 40s Protocol
At 40, the peptide conversation centers on perimenopause and the gradual GH axis decline. CJC-1295 with Ipamorelin is the most common entry point because the GH pulse pattern is what is failing first. At 50, the conversation centers on what has already happened: estrogen is gone, GH has dropped further, lean mass and bone are eroding, and the recovery system has slowed. The peptide mix shifts. Epithalon becomes more central. Tesamorelin appears more often because post-menopausal visceral fat patterns are more entrenched. Wolverine recovery work moves up the priority list because connective tissue healing is meaningfully slower. The 40s protocol is about catching the shift early. The 50s protocol is about restoring function in systems that have already changed.
Foundation First: What Must Be in Place Before Peptides After 50
Peptides do not work in isolation. At Perfect B in Doral we require four foundations before prescribing any protocol for a woman over 50. Skipping the foundation is the most common reason patients see disappointing results from peptide therapy and conclude the molecules do not work.
- Hormone status documented. Estradiol, FSH, thyroid panel, fasting insulin, IGF-1, vitamin D, and a complete metabolic panel. Women already on hormone replacement therapy need their levels reviewed and stable before adding peptides. Women in their 50s also benefit from a baseline DEXA scan if one has not been done in the past two years.
- InBody scan or equivalent body composition assessment. Visceral fat, skeletal muscle mass, and body water guide which peptide enters the protocol first. A scan replaces guesswork with a measurable starting point and gives us a baseline to measure against in twelve weeks.
- Resistance training, not just cardio. Muscle protein synthesis declines after menopause regardless of estrogen status. Walking is not enough. Loaded movement two to three times per week is the minimum input the protocol needs to work with, and the literature is consistent that strength training is the single most protective intervention against sarcopenia and bone loss after 50.
- Sleep and protein intake. Sleep below six hours and protein below approximately one gram per pound of lean mass will blunt every peptide on the menu. These are non-negotiable inputs, not optional optimizations. Many of the patients we see at our Doral clinic who self-describe peptide therapy as ineffective were under-sleeping or under-eating protein the entire time.
When these four are in place, peptide therapy becomes additive instead of compensatory. When they are not, even the right peptide produces underwhelming results and patients waste money on protocols that were set up to fail before they started.
The Peptides Perfect B Uses for Women Over 50, Organized by Goal
This is the actual Perfect B catalog for the post-menopausal patient. Each peptide has one or two primary clinical applications. Stacks are built by combining peptides whose goals do not overlap. We do not prescribe Sermorelin, PT-141, Kisspeptin, Gonadorelin, Selank, DSIP, Thymosin Alpha-1, or research-grade peptides sold online. For the broader female catalog across all ages, see our complete clinical guide to the best peptides for women organized by goal.
GHK-Cu: For Skin Atrophy, Collagen, and Visible Aging
GHK-Cu, the copper peptide, is the most commonly added peptide for women over 50 whose primary concern is visible skin change. Post-menopausal skin loses dermal density beyond simple wrinkling, what dermatologists call skin atrophy. GHK-Cu signals fibroblasts to upregulate collagen, elastin, and hyaluronic acid, and it supports wound healing and hair follicle regeneration. The effect is gradual and compounds over twelve weeks. According to a peer-reviewed clinical review in the National Library of Medicine summarizing GHK-Cu’s role in tissue remodeling and skin regeneration, the peptide has been documented in clinical research since the early 1970s and remains one of the most validated copper-binding peptides in dermatologic use.
CJC-1295 with Ipamorelin: For Sleep, Body Composition, and Energy
The CJC-1295 and Ipamorelin combination stimulates the natural release of growth hormone from the pituitary in a pulsatile pattern that mirrors physiology. After menopause, deep sleep is the first thing this combination tends to restore. Women in their 50s using this blend report deeper, more restorative sleep within two to three weeks, with body composition changes following over the next two to three months as the growth hormone pulse normalizes. For the perimenopausal version of this protocol see our clinical breakdown of why the growth hormone axis shifts after 35 in women and how it is addressed before menopause.
Wolverine Stack (BPC-157 with TB-500): For Recovery and Joint Comfort
Recovery is one of the underappreciated peptide categories for women over 50. Connective tissue heals slower after menopause. Workouts that used to require one rest day now require two. Old injuries flare up. The Wolverine stack pairs BPC-157, which supports gut lining and tendon repair, with TB-500, which supports broader tissue regeneration. The stack is particularly valuable for active women in their 50s who want to keep training without accumulating chronic injuries that compound over months.
Tesamorelin: For Post-Menopausal Visceral Fat and Metabolic Stall
Tesamorelin is the most direct option for the post-menopausal patient whose primary issue is stubborn visceral fat. Post-menopausal fat redistribution is real and not a willpower problem. As estrogen drops, fat shifts from the hips and thighs to the abdomen, and visceral adiposity rises even when total body weight is stable. Tesamorelin is a growth hormone releasing hormone analog originally FDA-approved for HIV-associated lipodystrophy and used clinically off-label for visceral adiposity in patients without that diagnosis. We reach for Tesamorelin specifically when InBody visceral fat readings are elevated, when the patient has tried foundation interventions without resolving the abdominal pattern, and when IGF-1 baseline labs make the protocol safe to initiate.
Epithalon: For Longevity, Sleep Architecture, and Pineal Function
Epithalon is the peptide that takes a more central role at 50 than it does at 40. It is a synthetic tetrapeptide modeled on a pineal-derived molecule and studied for decades by Russian gerontology researcher Vladimir Khavinson for its effect on age-related markers. Patients in their 50s typically run short cycles two to three times per year rather than continuously. The reported effects include deeper sleep, reset circadian rhythm, and gradual changes in skin texture that compound over multiple cycles. For the detailed clinical breakdown see our clinical guide to Epithalon and its role in longevity and sleep architecture. Long-term observational data is available in a longitudinal Khavinson study published in the National Library of Medicine examining Epithalon’s effect on age-related cellular markers over 12 years.
MOTS-c: For Cellular Energy and Mitochondrial Function
MOTS-c is a mitochondrially-derived peptide that supports cellular energy production, insulin sensitivity, and metabolic flexibility. It is one of the peptides whose mechanism becomes more relevant after 50 because mitochondrial dysfunction is a recognized contributor to post-menopausal fatigue, exercise intolerance, and weight gain. We use MOTS-c in protocols where energy and metabolic markers are the primary complaint and other peptides have already addressed sleep and recovery.
How Perfect B Decides Which Peptide for Which Patient
There is no template stack for women over 50 at Perfect B. The selection logic is structured but individualized. We use a documented criterion that combines the InBody scan with baseline labs and a symptom map.
- Visceral fat elevated, skeletal muscle adequate. Tesamorelin enters the protocol first, with the goal of reducing the visceral pattern before adding muscle-targeting peptides.
- Skeletal muscle low, visceral fat normal or borderline. CJC-1295 with Ipamorelin enters first, with sleep and lean mass as the primary endpoints.
- Both visceral fat elevated and skeletal muscle low. A blended protocol combining Ipamorelin and Tesamorelin is used, dosed for the dominant complaint first.
- Skin and connective tissue as the primary complaint. GHK-Cu enters the protocol, often alongside a low-dose growth hormone secretagogue if labs support it.
- Longevity and sleep as the central goal. Epithalon is added in short cycles, sometimes as the only peptide in the rotation for women whose body composition and skin are already in good standing.
- Joint and recovery complaints dominating. The Wolverine stack enters first, with body composition peptides added later if needed.
This is the actual decision process Valeria Marulanda follows in our Doral clinic. It is not a marketing framework. The criterion exists because in clinical experience the predictable failure mode for peptide therapy is prescribing the second-best peptide for a patient whose presentation pointed to a different first choice.
Peptides and Hormone Therapy After 50: Complementary, Not Competitive
Peptides for menopause are used to support sleep, body composition, and recovery, not to replace hormone therapy. The two protocols address different mechanisms, and the women who get the best results in their 50s typically run both rather than choosing between them.
Hormone replacement therapy addresses estrogen, progesterone, and in some protocols testosterone directly. It manages hot flashes, vaginal atrophy, mood, bone density, and cardiovascular markers tied to estrogen status. Peptides address upstream signaling, growth hormone pulse frequency, cellular repair, mitochondrial function, and connective tissue regeneration. The categories do not overlap. A woman on a stable HRT regimen who adds CJC-1295 with Ipamorelin is not duplicating treatment, she is layering two protocols that target different physiology.
The decision about whether to add peptides to an existing HRT regimen depends on what remains unaddressed. If sleep is still fragmented despite optimized estrogen and progesterone, that points to a growth hormone or pineal angle. If recovery and joint discomfort persist, that points to connective tissue work. If body composition has not responded to HRT plus exercise, that points to a growth hormone or visceral fat angle. The peptide answer is specific to what HRT has and has not solved.
Already on HRT and Considering Peptides? See What Patients at Your Stage Are Running.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
What Women in Their 50s at Our Doral Clinic Notice First
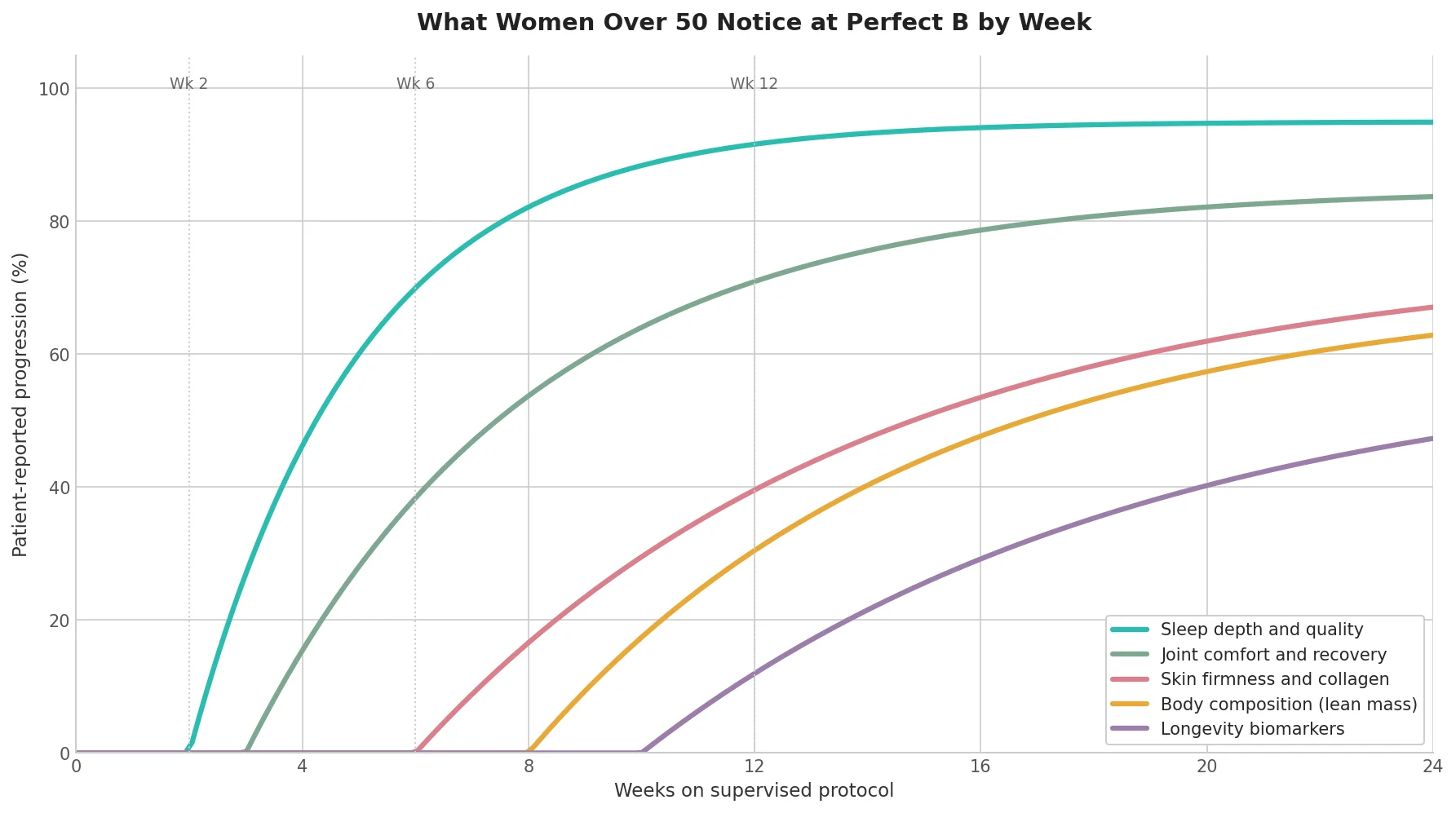
The timeline below reflects the typical sequence of changes patients in their 50s report at Perfect B on a properly structured protocol. It is not a guarantee. It is the pattern we have learned to expect when foundations are in place, labs support the choice, and the woman runs the protocol consistently.
- Weeks 1 to 2: Sleep depth. Deeper, more restorative sleep is the first change most patients report. Wake-ups during the night decrease and morning energy improves before any body composition change is visible.
- Weeks 3 to 6: Joint comfort and recovery. Workouts feel like they hit the same muscles harder without producing the same soreness afterward. Old joint complaints quiet down.
- Weeks 6 to 10: Skin and connective tissue. Texture, firmness, and elasticity improve gradually. Hair texture often follows. These are the changes friends and family notice before the patient does.
- Weeks 8 to 16: Body composition. Lean mass increases, visceral fat decreases, and clothes fit differently even when the scale moves less than expected. This is where InBody scans become useful, because the patient’s own perception lags behind the actual change.
- Weeks 12 and beyond: Longevity biomarkers. IGF-1 normalization, improved fasting insulin, and over multiple cycles, gradual shifts in markers tied to cellular aging. These are the changes that justify long-term cycled protocols rather than short trial runs.
The Cancer and IGF-1 Conversation Few Clinics Will Have
Most articles about peptides for women over 50 skip the cancer conversation entirely. We do not. Peptides that elevate IGF-1, including CJC-1295, Ipamorelin, and Tesamorelin, raise a legitimate question about hormone-sensitive and growth-sensitive cancer risk that women in their 50s should hear honestly before starting.
The available data is mixed and the long-term human studies do not exist at the scale that would settle the question. What is known is that IGF-1 is a growth signal, that some cancers respond to growth signals, and that women with a personal history of breast cancer, ovarian cancer, or any active malignancy are not candidates for growth hormone secretagogues regardless of how mild the protocol appears. The cautious approach for women in their 50s with a family history of hormone-sensitive cancers is to discuss the question with both the prescribing clinician and the woman’s oncologist or primary care provider before initiating any peptide that elevates IGF-1.
This is not a reason to avoid peptides as a category. It is a reason to be selective about which peptide and to document the conversation with the patient before the first injection. At Perfect B we explicitly contraindicate the growth hormone secretagogue category in patients with relevant cancer history, and we direct those patients toward GHK-Cu and Epithalon, whose mechanisms do not involve elevating IGF-1 in the same way.
What Peptides for Women Over 50 Will NOT Do
Honest expectations protect the protocol. There are five outcomes peptides will not deliver no matter which peptide is chosen, what the dose is, or how long the cycle runs.
- They will not replace hormone replacement therapy. Peptides do not contain estrogen, progesterone, or testosterone. They do not address vaginal atrophy, hot flashes, or bone density on the timeline HRT does.
- They will not produce facelift-level skin change in twelve weeks. GHK-Cu changes texture and firmness over months, not weeks. Anyone promising a visible lift is not describing peptide biology.
- They will not compensate for inadequate protein or sleep. A woman eating sixty grams of protein per day and sleeping five hours will not respond meaningfully to peptides. The foundation has to be in place.
- They will not turn back the calendar. The realistic frame is slowing the rate of decline and restoring function in specific systems, not reversing a woman in her 50s to her 30s.
- They will not work without supervision. Self-sourced peptides from online research-grade sellers do not have the active compound, sterility, or dosing accuracy required for clinical results.
Safety and Contraindications Women Over 50 Should Know
The categorical contraindications for peptide therapy in women over 50 are documented at Perfect B and reviewed at intake. The list below covers the conditions and medications that change whether the protocol is appropriate, not the conditions that simply require additional monitoring.
- Active or recent cancer. Especially hormone-sensitive cancers and any malignancy with growth-signal sensitivity. Growth hormone secretagogues are contraindicated. Some peptides may still be appropriate after clearance from the patient’s oncologist.
- Pregnancy or active breastfeeding. Not relevant for the typical post-menopausal patient but worth stating explicitly.
- Severe diabetic retinopathy or proliferative retinopathy. Growth hormone secretagogues can worsen this condition.
- Uncontrolled hypertension or active cardiovascular event. Stabilization first, peptides later if appropriate.
- Specific medication conflicts. Insulin sensitizers, GLP-1 medications already in use, and certain blood thinners require dose review before adding peptides. The interaction is not always a contraindication but it changes the protocol.
How to Start at Perfect B: Consultation, Labs, InBody Scan
The intake process for a woman over 50 considering peptide therapy at our Doral, FL clinic follows the same sequence every time. The structure exists because each step informs the next, and skipping a step is the most common reason patients end up on the wrong protocol.
- Initial consultation. A conversation about goals, history, current HRT or medication use, family history of hormone-sensitive cancers, and what foundations are already in place.
- Labs. Estradiol, FSH, thyroid panel, fasting insulin, IGF-1, vitamin D, complete metabolic panel, and any additional markers relevant to history.
- InBody scan. Visceral fat, skeletal muscle mass, total body water, and segmental analysis. This is the measurement that turns a goal conversation into a protocol decision.
- Protocol design. The peptide or stack is chosen against the InBody and lab picture, not against the patient’s preference for a specific compound she read about online.
- First cycle and follow-up. Typically four to twelve weeks depending on the peptide. Labs and InBody are repeated to verify the protocol is producing the expected change before continuing.

See What Women Patients in Their 50s With Similar Labs Are Running at Perfect B in Doral.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
Frequently Asked Questions
1. What is the best peptide for women over 50?
There is no single best peptide for women over 50. The right choice depends on the primary goal. For skin and visible aging, GHK-Cu is most often the first choice. For sleep, body composition, and energy, CJC-1295 with Ipamorelin is the most common starting point. For visceral fat and metabolic stall, Tesamorelin is the most direct option. For longevity and sleep architecture, Epithalon takes a central role at 50 that it does not have at 40. At Perfect B in Doral, FL the catalog is chosen by goal and validated with an InBody scan and baseline labs.
2. Should menopausal women take peptides?
Peptides can be appropriate for many women in their 50s but they are not appropriate for every woman. They are not a substitute for hormone replacement therapy and they require foundations like resistance training, adequate protein, and sleep to be in place. They are contraindicated in women with active or recent hormone-sensitive cancers, in pregnancy, and in several specific medical conditions. The honest answer is that peptides can be a strong addition to a supervised post-menopausal protocol when the clinical picture supports them, and a poor choice when foundations are missing or contraindications are present.
3. What should you not mix peptides with?
The most clinically relevant interactions for women over 50 involve insulin sensitizers, GLP-1 medications like semaglutide or tirzepatide already in use, certain blood thinners, and corticosteroids. None of these are automatic exclusions but each one changes the protocol design and dose adjustment. Alcohol in significant or daily amounts will blunt growth hormone secretagogue results. Sleep medications that suppress deep sleep architecture will interfere with the sleep-driven mechanism of CJC-1295 with Ipamorelin and Epithalon. The decision about what to layer or avoid is made during the consultation with the full medication list in front of the prescriber.
4. Which peptide is best for sagging skin after 50?
GHK-Cu is the peptide most directly aimed at collagen synthesis and skin firmness. It can be used as a topical formulation, as a microneedling adjunct, or as an injectable depending on the clinical indication. For women in their 50s whose primary complaint is skin laxity, the realistic expectation is gradual improvement in texture and firmness over twelve weeks, not a visible facial lift. Combining GHK-Cu with in-clinic procedures that stimulate collagen mechanically, such as microneedling or radiofrequency, produces faster visible change than peptide alone.
5. Can women over 50 take peptides with hormone replacement therapy?
Yes, in most cases. Peptides and HRT address different mechanisms and the two protocols are commonly layered in women in their 50s. The qualifier is that HRT levels should be stable and documented before adding peptides, and the prescribing clinician needs the full picture to design the combined protocol safely. Women with a history of hormone-sensitive cancers on HRT for narrow indications require additional discussion before adding any peptide that elevates IGF-1.
6. How long does it take to see results from peptides at 50?
The first noticeable change is typically sleep depth within two to three weeks on a CJC-1295 with Ipamorelin or Epithalon protocol. Recovery and joint comfort follow at three to six weeks on the Wolverine stack. Skin and connective tissue changes appear at six to ten weeks on GHK-Cu. Body composition shifts at eight to sixteen weeks on Tesamorelin or growth hormone secretagogues. Longevity biomarkers shift over multiple cycles spanning several months. Patients who run a protocol for four weeks and stop typically do not see the changes that show up later in the timeline.
7. How does Perfect B decide which peptide is right for a woman over 50?
The selection follows a documented criterion that combines the InBody scan, baseline labs (including estradiol, FSH, IGF-1, fasting insulin, thyroid, vitamin D, and a metabolic panel), and a symptom map. Visceral fat elevated points to Tesamorelin. Skeletal muscle low with normal visceral fat points to CJC-1295 with Ipamorelin. Both compromised points to a blended Ipamorelin and Tesamorelin protocol. Skin as the primary complaint points to GHK-Cu. Recovery as the primary complaint points to the Wolverine stack. Longevity and sleep as the central goal points to Epithalon.
Closing: The Clinic Takeaway on Peptides for Women Over 50
The honest answer to which peptides are best for women over 50 is that the answer depends on what is failing first. Sleep and recovery, skin and connective tissue, visceral fat and lean mass, longevity markers, and cellular energy each have a different peptide answer, and the choice is made against an InBody scan and labs rather than against a wish list. The biology after 50 is not the biology at 40, and a protocol designed for a perimenopausal patient is not automatically right for a post-menopausal patient fifteen years past her last cycle.
What separates a peptide protocol that works from one that disappoints is the supervision layer. The right molecule from a licensed compounding pharmacy, dosed against documented labs, layered with foundations that the patient is actually doing, and monitored across cycles is a different intervention from a vial purchased online and injected on a guess. At Perfect B in Doral, FL the supervision is the product.
- 📍 Visit us at Perfect B | 3905 NW 107th Ave, Suite 104, Doral FL 33178
- 📞 Call or message us at (786) 502-2260
- 💳 Buy Now Pay Later available: Cherry, Klarna, Afterpay, CareCredit
→ Book your peptide consultation at Perfect B in Doral today.


