

Perfect B, Doral FL. | 06.05.26 | 10 min read.
This content is for educational purposes only and does not constitute medical advice. Acne treatment requires individualized clinical evaluation. Results vary by skin type, hormonal status, and treatment adherence. Consult a licensed medical provider before beginning any acne treatment protocol.
Teen Acne and Adult Acne Look the Same on the Surface. Clinically, They Are Not.
Acne affects approximately 50 million Americans annually. It is the most common skin condition in the United States. But the assumption embedded in most over-the-counter products and even some clinical protocols is that acne is acne: clogged pores, excess oil, bacteria. Treat the oil, clear the pores, done. That assumption is wrong, and in patients over 35, acting on it consistently makes the skin worse.
Teen acne and adult acne share surface-level similarities: papules, pustules, and comedones appear in both populations. But the hormonal driver behind each is fundamentally different. The skin itself is different. The way breakouts heal is different. And critically, the treatment approach that works for one can actively harm the other. At Perfect B in Doral, FL, the clinical distinction between these two presentations shapes every acne protocol from the first consultation forward.

Key Takeaways
- Teen acne is driven by androgen surges during puberty that flood the T-zone with excess sebum. The skin is thick, resilient, and heals quickly. Aggressive protocols are tolerated well.
- Adult and perimenopausal acne is driven by estrogen decline while androgens remain relatively elevated. Breakouts concentrate along the jawline and neck. The skin barrier is thinner, drier, and heals slowly, leaving post-inflammatory hyperpigmentation that persists for months.
- The most common clinical error in adult acne is applying a teen-grade protocol to a compromised barrier. Benzoyl peroxide at high strength, aggressive salicylic acid peels, and harsh cleansers strip the lipid barrier and trigger a rebound sebum surge that worsens breakouts.
- Perimenopausal patients often present with a paradox: skin that looks oily and feels flaky at the same time. This is barrier dysfunction, not excess sebum. Treating it as a teen acne problem is the most reliable way to make it worse.
- At Perfect B in Doral, the in-clinic sequencing rule for adult acne with scarring is: calm the active inflammation for six weeks first, then introduce microneedling or RF microneedling for scars. Treating scars over an active flare produces no improvement and risks spreading inflammation.
The Hormonal Driver Is Completely Different in Every Age Group
In Teens: Androgens Surge and Sebum Overflows
During puberty, rising androgen levels stimulate the sebaceous glands to produce significantly more oil than the skin can process. The result is a T-zone overflow: forehead, nose, and chin become visibly oily, pores fill with sebum and dead skin cells, and Cutibacterium acnes (formerly P. acnes) proliferates in that anaerobic environment. The breakouts that follow are the body’s inflammatory response to that bacterial overgrowth, not a disorder of the skin barrier itself.
Teen skin is thick, has a strong lipid barrier, and regenerates quickly. Post-inflammatory marks fade within weeks. This combination means the skin can tolerate, and often requires, more aggressive intervention: higher-strength benzoyl peroxide, salicylic acid peels, and, when needed, oral antibiotics or isotretinoin. The skin’s resilience is the asset.
In Adult Patients 30s to 40s: Hormonal Cycling Shifts the Pattern
Adult acne affects roughly 25% of men and up to 50% of women in their 20s and 30s. The driver is no longer a global androgen surge but a more targeted hormonal imbalance, often tied to the menstrual cycle, stress-induced cortisol, polycystic ovarian syndrome, or lifestyle factors like protein supplement use and testosterone supplementation. The breakouts in this population are more commonly inflammatory: papules, pustules, and nodular cysts along the jawline, lower cheeks, and sometimes the back and shoulders. They do not resolve as quickly as teen breakouts, and they leave hyperpigmentation that can persist for months on darker skin tones.
In Perimenopausal Patients 40s and Beyond: Estrogen Drops While Androgens Hold
The perimenopausal transition introduces a different hormonal dynamic. Estrogen begins to decline, and with it goes much of the hormonal balance that had kept androgens in check. The relative androgen excess that results drives sebaceous activity, but the skin environment in which this happens is completely different from teen skin. The lipid barrier is thinner. Collagen production has slowed. The skin’s moisture-retaining capacity is reduced. The result, as Victoria Diartt observes consistently in clinic, is a confusing presentation: skin that looks oily in the T-zone and flaky around the cheeks and temples at the same time, with cystic breakouts along the jawline that do not respond to the products the patient has been using since her 20s. A 2023 narrative review in the Anais Brasileiros de Dermatologia comparing adolescent and adult acne across epidemiology, pathophysiology, and treatment confirms that adult-onset acne is driven by a different hormonal mechanism than adolescent acne and requires modified treatment approaches, particularly regarding retinoid selection and barrier preservation.
Where the Breakouts Appear and Why That Location Is Clinically Significant
Teen Acne: T-Zone Dominance
Teen breakouts concentrate in the T-zone because that region has the highest sebaceous gland density in adolescent skin. Forehead, nose, and chin develop blackheads, whiteheads, and papules first. The cheeks may be involved in moderate to severe cases, but the primary zone is the central face. This T-zone pattern is consistent enough that it functions as a clinical indicator: when a younger patient presents with T-zone dominant acne, the protocol centers on sebum reduction and comedolytic agents.
Adult Acne: Jawline and Lower Face
Adult hormonal acne overwhelmingly favors the jawline, lower cheeks, chin, and neck. This distribution reflects the androgen receptor density in the lower face, which responds disproportionately to hormonal fluctuations. In male patients, the pattern often extends to the back and shoulders. In perimenopausal women, the jaw and neck are the primary sites, with some patients developing breakouts that extend onto the chest during high-stress periods. The T-zone may be relatively clear.
This location shift matters beyond diagnosis. It means that products and protocols designed to address T-zone sebum excess are being applied to a lower face where the problem is hormonal and the skin barrier is already under stress, not to an oily zone that needs to be dried out. → The complete clinical breakdown of perimenopausal acne at Perfect B in Doral, FL, including what triggers the lower-face pattern and why it responds to barrier repair instead of drying protocols, is covered in the acne after 40 guide.

How the Skin Itself Changes Between Adolescence and Perimenopause
Teen Skin: Thick, Resilient, and Forgiving
The defining characteristic of adolescent skin from a treatment standpoint is its resilience. High collagen density, a robust lipid barrier, strong cell turnover, and a well-functioning moisture retention system mean that teen skin can absorb aggressive treatment without structural damage. A patient at 16 who over-applies benzoyl peroxide may experience dryness and irritation, but the skin recovers quickly. Post-inflammatory marks from healed breakouts typically fade within two to four weeks. This resilience justifies a more aggressive approach when the acne severity warrants it.
Adult 40+ Skin: Thinner Barrier, Lipid Loss, Slower Healing
By the time a patient is in their 40s, the skin has lost a significant portion of its lipid content, collagen density has declined, and the natural cell turnover rate has slowed. The skin barrier, which in a teenager functions as a near-impermeable shield, is now thinner and more permeable. This is normal biological aging, not a pathology. But it means that the same acid concentration that a teenager’s skin handles without incident can strip a 40-year-old’s barrier and trigger a cascade: the barrier breakdown causes increased transepidermal water loss, the skin becomes reactive and inflamed, the sebaceous glands respond by producing more sebum to compensate, and the acne gets worse. The cause appears to be product sensitivity, but the actual mechanism is barrier disruption.
Why Post-Inflammatory Hyperpigmentation Persists Longer in Adult Patients
In teen patients, the high cell turnover rate means post-inflammatory hyperpigmentation from a resolved breakout typically fades within weeks. In adult patients, the slower turnover extends that timeline to months. In patients with Fitzpatrick III to VI skin, which represents the majority of the South Florida and Doral patient population at Perfect B, both the intensity of PIH and its persistence are amplified. A 40-year-old patient with Fitzpatrick IV skin who develops a deep cystic breakout along the jawline and is treated with an inappropriate acid protocol may find that the post-inflammatory mark outlasts the acne itself by three to six months. This is why the treatment approach in this population prioritizes inflammation containment and barrier integrity from the start, not just clearing the active lesion.
The Clinical Comparison: How Teen and Adult Acne Differ Across Six Dimensions
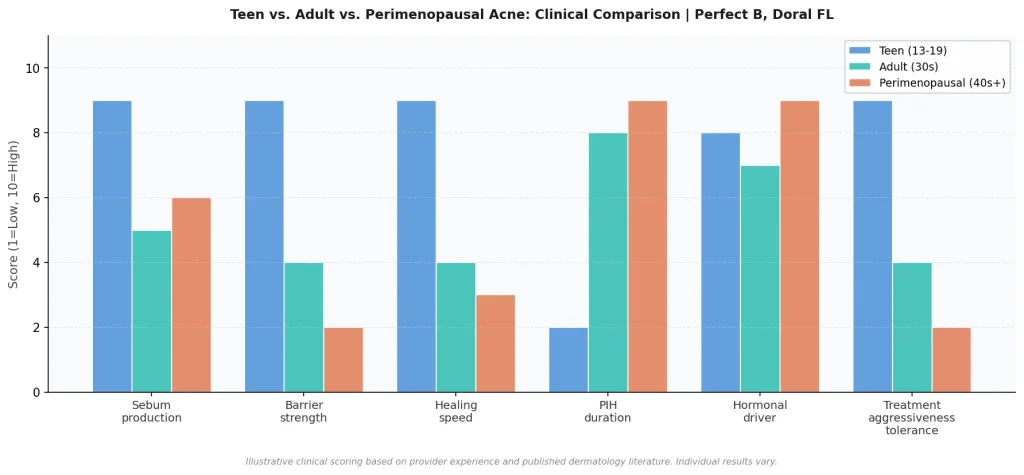
Why Treating Teen Acne and Adult Acne the Same Way Makes Things Worse
The most common clinical pattern Victoria Diartt sees in new adult acne patients is not untreated acne. It is acne that has been aggressively treated with products designed for teenage skin. High-strength benzoyl peroxide washes, prescription-grade salicylic acid at concentrations appropriate for a 16-year-old, or multiple active ingredients layered together. The skin is stripped of its lipid barrier. It becomes sensitized, reactive, and paradoxically oilier as the sebaceous glands compensate for the moisture loss. The patient interprets the increased oiliness as a sign the acne is getting worse and uses more product. The cycle accelerates.
The perimenopausal patient who presents with both oily-looking skin and flaky patches is experiencing this barrier dysfunction in real time. The oiliness is rebound sebum, not baseline sebum excess. The flakiness is the visible sign of lipid loss. The acne breakouts are happening on a barrier that is already compromised. Half of the clinical work at Perfect B in this population is reversing what the wrong protocol has done before any active treatment for the acne can begin.
“The skin at 45 just wants to be soothed, not punished,” Victoria observes. “Once patients understand that the ‘dry it out’ approach is the thing that’s keeping them stuck, the turnaround is dramatic.” This insight is the foundation of the adult acne protocol at Perfect B. The goal is not to eliminate oil. The goal is to restore barrier function, reduce inflammation, and then address the hormonal driver with targeted interventions that the barrier can tolerate.
How the Treatment Protocol Differs at Every Stage of Life
Teen Protocol: Clarify, Control Sebum, Tolerate Aggression
For teen patients at Perfect B, the in-clinic approach centers on deep pore cleansing and sebum control. A clarifying HydraFacial with a salicylic acid boost is the primary treatment, targeting blackheads, comedones, and active papules while the vortex extraction removes impacted sebum without manual extraction trauma. If the skin can tolerate it and the acne severity justifies it, a light salicylic acid or mandelic acid peel follows to accelerate cell turnover. At-home, the protocol is straightforward: a benzoyl peroxide gel in the morning, a gentle non-comedogenic cleanser morning and evening, and a retinoid at night if the severity warrants it.
Adult 30s to 40s Protocol: Targeted Topicals, Hormonal Awareness
For adult patients in their 30s and 40s, the in-clinic and at-home approach is built around precision rather than strength. In clinic, a gentle peel appropriate for the patient’s Fitzpatrick type and current barrier status. For darker skin types, a mandelic or lactic acid peel rather than salicylic at high concentration. At-home, the combination Victoria uses is tretinoin at night buffered over a ceramide moisturizer to prevent irritation, a clindamycin-benzoyl peroxide gel in the morning, and a gentle low-pH cleanser that does not strip the barrier. When a male patient in this age group discloses testosterone supplementation or mentions whey protein as a dietary staple, the protocol is adjusted to account for the androgen-driven sebum contribution. Those conversations happen at every consultation. The clinical picture is incomplete without them.
Perimenopausal Protocol: Barrier First, Inflammation Second, Scars Third
For perimenopausal patients, the sequence is non-negotiable: repair the barrier first, then address the active inflammation, then address any residual scarring. In clinic, a gentle enzyme peel or red LED to reduce inflammation without acid stress on a compromised barrier. At home, ceramides and niacinamide as foundational ingredients before any active treatment is layered on top. Retinoids enter the protocol only once the barrier has stabilized, at low concentration and buffered over moisturizer. Microneedling for scars is introduced only when there are no active flares, typically after six weeks of inflammation management. Treating scars during an active flare produces no measurable improvement and risks spreading the inflammatory response to adjacent tissue. → The full protocol for microneedling for acne scars at Perfect B in Doral, FL, including the sequencing rules, SkinPen vs Morpheus8 selection by scar type, and the exosome stacking option for perimenopausal patients, is covered in the microneedling for acne scars guide.

Fitzpatrick Type Changes the Equation, Especially in South Florida
The Fitzpatrick type consideration applies to both teen and adult patients but is most consequential in adult and perimenopausal cases, where the skin barrier is already under stress. In Miami and Doral, the patient population at Perfect B is predominantly Fitzpatrick III to VI: Hispanic, Caribbean, and Brazilian patients whose skin has higher melanin density and a proportionally higher risk of post-inflammatory hyperpigmentation from acne and from aggressive treatment.
For a teen patient with Fitzpatrick IV skin, the acid concentration for in-clinic peels is reduced and a tyrosinase inhibitor is incorporated in the pre-treatment protocol to prevent PIH from the peel itself. For a perimenopausal patient with Fitzpatrick V skin presenting with active jaw acne and a compromised barrier, the conservative approach is not optional. High-acid peels in this context would produce PIH that outlasts the acne by months. The in-clinic protocol defaults to enzyme peels, LED, and barrier-repair ingredients. A clinical overview from Clearview Dermatology notes that adult acne affects up to 50% of women in their 20s and 30s and that treatment approaches differ significantly between age groups due to varying causes and skin sensitivity, reinforcing the need for age-specific rather than severity-specific protocols. → The complete guide to chemical peels for acne at Perfect B in Doral, FL, including peel type selection by Fitzpatrick type and concentration adjustments for darker skin tones, is available in the chemical peel for acne guide.
Frequently Asked Questions
1. Can you have both teen-type and adult-type acne at the same time?
Yes, and it is more common in patients in their early 20s who are still experiencing some residual sebum-driven T-zone breakouts while also developing the hormonal jawline pattern that characterizes adult acne. In these cases the clinical approach requires addressing both drivers simultaneously: a comedolytic strategy for the T-zone and a hormone-aware, barrier-protective strategy for the jaw. The protocols run in parallel but are not identical.
2. Why does my acne keep getting worse in my 40s even though I have always had clear skin?
Adult-onset acne in patients who had no significant acne history as teenagers is often a direct consequence of the perimenopausal hormonal shift. Estrogen decline removes a hormonal counterweight that had been suppressing androgen-driven sebum activity for decades. The sebaceous glands respond to the relative androgen increase by becoming more active, at the same time as the skin barrier is losing lipid density and the skin’s repair capacity is slowing. The combination produces breakouts that feel nothing like teen acne and respond to an entirely different treatment approach.
3. Is benzoyl peroxide safe for adult acne?
In lower concentrations (2.5% to 5%) combined with a moisturizer and a barrier-supportive routine, benzoyl peroxide can be appropriate for adult acne, particularly when used in the morning as part of a clindamycin-BPO combination. At higher concentrations, used without adequate moisturization on a compromised adult barrier, BPO is one of the most reliable ways to destabilize the skin and trigger a rebound sebum response. The concentration, vehicle, and surrounding routine matter as much as the ingredient itself.
4. How long does adult acne treatment take to work compared to teen acne?
For teen patients on an appropriate protocol, visible improvement in new breakout frequency typically appears within four to six weeks. Comedone clearance may lag behind by a few weeks. For adult and perimenopausal patients, the same four-to-six-week window applies for reduction in active breakouts, but the post-inflammatory hyperpigmentation from existing marks can take three to six months to fade, particularly in Fitzpatrick III to VI skin. Any scarring that developed during the period of acne activity requires a separate treatment timeline, beginning only once active breakouts are controlled.
5. Can diet affect teen acne and adult acne differently?
Diet affects both populations through the same mechanisms: high glycemic load foods spike insulin and IGF-1, both of which stimulate sebaceous gland activity. Dairy, especially whey protein, has the most consistent clinical association with acne across age groups. In adult male patients, protein supplements derived from whey are a consistent trigger that is often overlooked until specifically asked about. The impact of dietary changes is real in both teen and adult acne, but the overall contribution to adult hormonal acne is proportionally smaller than the hormonal driver itself. Diet modification is part of the protocol, not a replacement for targeted treatment.
6. Does microneedling help with both teen and adult acne scars?
Microneedling for acne scars is appropriate for both teen and adult patients once active acne is under control. The timing rule applies regardless of age: no microneedling over an active flare. The device selection varies by scar type and skin Fitzpatrick type. For teen patients with rolling or boxcar scars on Fitzpatrick II to III skin, SkinPen at appropriate depth is typically the first option. For adult and perimenopausal patients with mixed scar types on Fitzpatrick IV to VI skin, Morpheus8 RF microneedling with precise depth and energy control gives better outcomes and reduces the PIH risk from superficial needle trauma. Results for either protocol take three to six months to become fully visible.
The Skin at 45 Is Not the Skin at 15. The Treatment Plan Should Not Be Either.
The clinical distinction between teen acne and adult acne is not a nuance. It is the difference between a treatment that clears the skin and one that destabilizes it further. The hormonal driver, the skin barrier, the healing timeline, and the risk of post-inflammatory hyperpigmentation are all fundamentally different between these two presentations. Applying a protocol built for one to the other is the most common clinical mistake in acne management, and it is one that patients continue making for years before they understand why nothing is working.
At Perfect B in Doral, FL, every acne consultation begins with the same question: which version of this condition are we actually treating? The answer determines everything that follows, from the peel concentration to the moisturizer to the sequencing of scar treatment. A supervised clinical plan built for the right hormonal context and the right skin barrier status is what produces durable clearance. The right information is the first step toward it.
📍 Perfect B | 3905 NW 107th Ave, Suite 104, Doral FL 33178
📞 Call or message us at (786) 502-2260 to schedule your acne consultation with a licensed medical provider.
💳 Buy Now Pay Later: Cherry, Klarna, Afterpay, CareCredit


