

Perfect B, Doral Fl. | 05.07.26 | 8 min read.
This post is for educational purposes only and does not substitute for personalized medical advice. Chemical peel protocols vary based on skin type, acne severity, and individual health history. Consult a licensed medical provider before beginning any chemical exfoliation treatment.
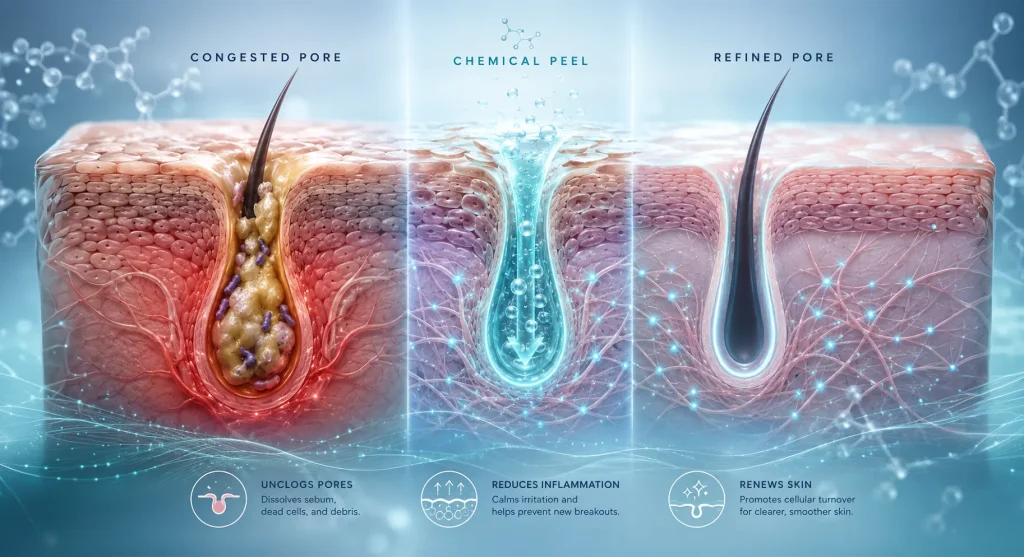
What Does a Chemical Peel Actually Do Inside Your Pore?
A chemical peel works by applying an acidic solution to the skin, which causes controlled injury to the epidermal layers. That injury triggers cellular turnover: the damaged skin sheds and new, healthier cells rise to replace it. For acne-prone skin, the mechanism is more specific than simple exfoliation. Certain acids are oil-soluble, which means they penetrate the lipid layer of the pore wall itself rather than just buffing the surface. That is how they reach the sebum, dead cells, and bacteria causing the problem.
The depth of a peel refers to how far the acid penetrates into the skin layers. Superficial peels work within the epidermis only. Medium-depth peels reach into the upper dermis. Deep peels go further still, but are rarely appropriate for acne management and carry significant risk on darker skin tones. At our clinic in Doral, FL, we work almost exclusively in the superficial to light-medium range for acne, which is where the clinical benefit is real and the risk of post-inflammatory hyperpigmentation is manageable.
Superficial vs medium depth: how the decision gets made
Depth selection is driven by three variables: acne type, skin tone, and inflammation status. Mild comedonal acne with minimal redness can tolerate a slightly deeper superficial peel. Active inflammatory acne with cysts or papules should only receive a light superficial approach. Going aggressive on inflamed skin does not accelerate clearing: it adds trauma to tissue that is already stressed and increases the risk of scarring and pigment damage.
Key Takeaways
- Salicylic acid is the clinical standard for oily, comedonal acne because it is oil-soluble and penetrates directly into the pore to clear congestion.
- Mandelic and lactic acid peels are safer for inflamed acne and darker skin tones due to their anti-inflammatory properties and lower risk of triggering post-inflammatory hyperpigmentation.
- Active cystic acne is a contraindication for peels: the inflammation must be controlled internally before any surface treatment begins.
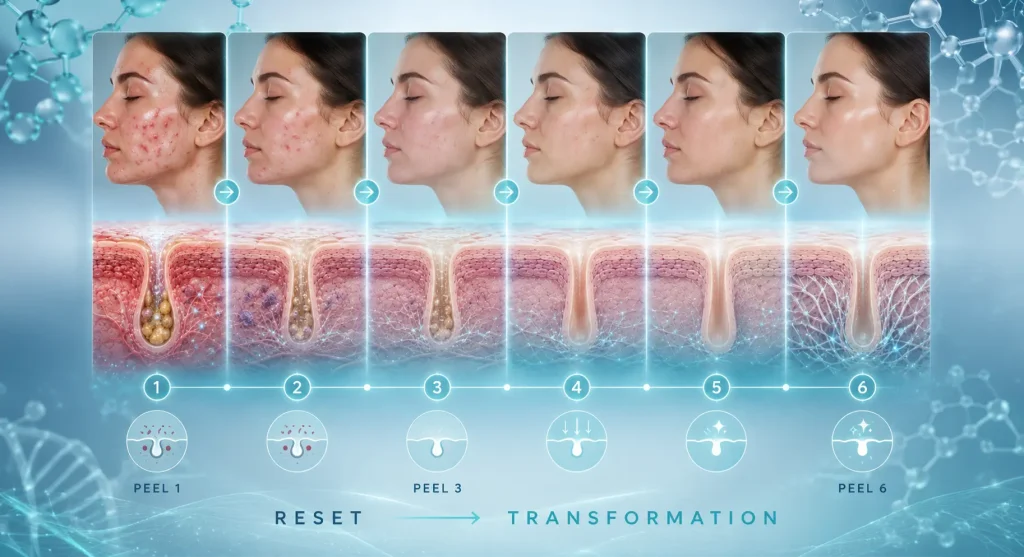
- A series of 4 to 6 peels spaced 3 to 4 weeks apart produces cumulative results that a single session cannot achieve. One peel is a reset. Four is a transformation.
- Medical clinic peels use higher acid concentrations with proper skin prep and Fitzpatrick assessment, which separates them from spa treatments and makes them appropriate for South Florida skin types.
Which Chemical Peel Is Right for Your Type of Acne?
The most common mistake in chemical peel selection is treating acne as a single condition. It is not. Oily comedonal acne, inflammatory papular acne, cystic acne, and post-acne pigmentation each respond differently to different acid types. Choosing the wrong one does not just fail to help: it can worsen inflammation, trigger hyperpigmentation, or damage a compromised barrier.
Salicylic acid: the go-to for oily skin and active breakouts
Salicylic acid is a beta-hydroxy acid (BHA) and it is oil-soluble. That property is what makes it the right choice for oily, congested acne. Unlike alpha-hydroxy acids, which work on the surface, salicylic acid gets into the pore lining and clears the sebum and debris driving the breakout. At Perfect B, we use salicylic acid peels for patients with active oily breakouts and comedonal congestion. Beyond clearing pores, salicylic has a mild anti-inflammatory effect that reduces the redness accompanying active lesions. It also loosens dirt from follicles and temporarily reduces oil secretion, which is why patients with oily skin notice reduced shine and smaller-looking pores after a series.
Mandelic and lactic acid: anti-inflammatory options for inflamed acne and darker skin tones
When a patient presents with heavily inflamed acne, lots of redness, and pustular lesions, we lean toward mandelic or lactic acid rather than salicylic. Both are alpha-hydroxy acids, but mandelic has a larger molecular size than glycolic, which means it penetrates more slowly and with less irritation. That gentleness makes it well suited for inflamed acne where the skin barrier is already compromised. Lactic acid is similarly gentle and has the added benefit of being a natural moisturizing factor, which keeps the barrier from becoming excessively dry during treatment. Both are significantly safer on Fitzpatrick III, IV, and V skin tones, which describes a large portion of our patient population in the Miami area. On darker skin, the risk of post-inflammatory hyperpigmentation (PIH) is real, and the last thing we want is to trade one discoloration problem for another.
Glycolic acid: post-acne brightness and texture improvement
Glycolic acid has the smallest molecular size of all the AHAs, which allows it to penetrate more deeply and produce more pronounced brightening and resurfacing. It is less targeted for active acne than salicylic but excellent when the goal shifts from clearing breakouts to improving overall skin texture, evening tone, and addressing the dullness and rough patches that often follow acne. We typically introduce glycolic as part of a maintenance series once active breakouts are controlled.
TCA: when you are targeting acne scars
Trichloroacetic acid (TCA) is a medium-depth peel agent that reaches into the upper dermis. It is not our first-line choice for active acne, but for patients dealing with atrophic acne scars or deeper textural damage, a properly dosed TCA peel can initiate collagen remodeling that lighter peels cannot. TCA requires careful patient selection, especially on darker Fitzpatrick types, and should only be performed by a medical provider who can assess the risk of PIH and manage the recovery period. Interest in TCA chemical peels for acne has grown substantially year over year, driven largely by patients researching more aggressive scar treatment options.

Does Your Fitzpatrick Skin Type Change the Chemical Peel Protocol?
Yes, significantly. The Fitzpatrick scale classifies skin from Type I (very fair, always burns) to Type VI (deeply pigmented, never burns). Types I through III tolerate more aggressive chemical exfoliation with less risk. Types IV through VI require a more conservative approach because melanocytes in darker skin are more reactive to injury, including the controlled injury of a chemical peel. When you stimulate those melanocytes without adequate caution, the skin produces excess melanin in response to the trauma, and you end up with post-inflammatory hyperpigmentation that can be as difficult to treat as the original acne scarring.
Why South Florida patients get a more conservative assessment
The patient population at our clinic in Doral reflects the demographic reality of South Florida: a high proportion of Hispanic, Caribbean, and Latin American patients who fall into Fitzpatrick III to V. This is not a minor consideration in our peel protocols. It is the starting point. Before any chemical peel, we assess Fitzpatrick type, recent sun exposure, any history of PIH, and the patient’s current melanin activity. For Type IV patients, we prefer mandelic acid at shallower depths, pre-treat with depigmenting agents when indicated, and apply more conservative timing during the procedure. This is not overcaution: it is the difference between a peel that clears acne and one that replaces it with a different pigment problem. A peer-reviewed review published in the Journal of Clinical and Aesthetic Dermatology documenting chemical peel safety and efficacy across skin types and the key role of Fitzpatrick classification in protocol selection supports this clinical approach.
When a Chemical Peel Is the Wrong Choice for Your Acne
Knowing when not to peel is as important as knowing which acid to use. Several conditions make chemical peels either ineffective or actively harmful for acne management, and a medical provider who skips this assessment is doing the patient a disservice.
Active cystic acne: calm the inflammation first
Cystic acne involves deep, nodular lesions with significant inflammation below the skin surface. Applying a chemical peel over active cysts does not accelerate healing. It adds surface trauma to already-inflamed tissue, increases the risk of rupture and scarring, and can spread bacteria to adjacent follicles. At Perfect B, if a patient presents with active cystic acne, we address the inflammation internally first before considering any surface treatment. The peel comes after the biology is calmer, not before. → Learn how Perfect B’s medical acne treatment plan in Doral, FL addresses active cystic acne and inflammatory breakouts before chemical exfoliation is introduced.
Accutane and retinoids: your barrier is too fragile
Patients currently using isotretinoin (Accutane) or high-strength topical retinoids are not candidates for chemical peels. These medications thin and sensitize the skin barrier, and adding a chemical exfoliant creates a risk of severe irritation, prolonged healing, and scarring. The standard guideline is to wait at least six months after completing isotretinoin before any chemical peel. With strong retinoids, we require a two-week minimum pause before treatment. Patients who do not disclose retinoid use before a peel are a common source of adverse outcomes in non-medical settings.
The Miami sun exposure problem
Miami’s UV index is consistently among the highest in the continental United States. After a chemical peel, the newly exposed skin is highly photosensitive, and unprotected sun exposure within the first week is one of the most reliable ways to trigger hyperpigmentation and undo the results of treatment. We require patients to avoid direct sun for a minimum of one week post-peel, use mineral sunscreen only (not chemical filters), and avoid high-sweat outdoor activities. Our specific guidance for Miami patients: no sweaty outdoor brunches, no outdoor workouts, no beach exposure. Miami’s humidity also creates a bacterial environment that can compromise healing if the skin is not kept clean and protected.
How Many Chemical Peels Do You Actually Need to Clear Acne?
A single peel produces visible improvement. Most patients notice brighter, smoother skin within a week of their first session, reduced congestion, and pores that feel cleaner. But a single peel is a reset, not a resolution. Real acne control through chemical exfoliation is cumulative, and the mechanism explains why: each peel accelerates cellular turnover, reduces the population of blocked follicles, and, over successive sessions, begins to remodel the skin architecture at a level one treatment cannot reach.
The 4-to-6 series: one peel is a reset, four is a transformation
Our standard protocol for acne management is a series of 4 to 6 peels, spaced 3 to 4 weeks apart. The spacing allows the skin to complete a full cellular turnover cycle between sessions, maximizing the benefit of each treatment. By the third peel, most patients with mild to moderate acne are seeing significant reduction in active breakouts and improved texture. By the fourth, the cumulative effect on pore congestion, tone, and overall skin quality is substantially different from what a single session produces. For patients with post-acne scarring or more significant hyperpigmentation, the series extends toward six sessions, sometimes with acid type adjusted partway through based on how the skin responds.
Chemical Peels for Post-Acne Dark Spots and Hyperpigmentation
Post-inflammatory hyperpigmentation (PIH) is one of the most common complaints from acne patients, particularly those with Fitzpatrick III to V skin tones. The acne resolves but the dark marks persist for months, sometimes longer. Chemical peels accelerate the turnover of pigmented cells at the surface level, gradually fading the marks. But at Perfect B, we rarely use peels alone for PIH. The more effective approach combines chemical exfoliation with agents that suppress melanin production at the source. Acne leaves, but the marks do not have to stay.
Adding tyrosinase inhibitors to shut down pigment production
Tyrosinase is the enzyme responsible for melanin synthesis. When it is overactivated by inflammation or injury, the skin produces excess pigment at the site of that injury, which is precisely how PIH forms. Tyrosinase inhibitors block this pathway at the enzymatic level. Tranexamic acid is one of the most effective and well-tolerated options in this category, and we commonly combine it with our peel protocols when PIH is a significant concern. The peel removes existing pigmented cells at the surface. The tranexamic acid prevents the melanocytes from producing new excess melanin in response to the treatment itself. The combination produces faster, more durable pigment clearance than either approach alone. → Learn how Perfect B’s brightening treatment plan in Doral, FL combines clinical-grade peels with targeted depigmenting protocols for post-acne hyperpigmentation.
What to Expect After a Chemical Peel in Miami
Recovery from a superficial to light-medium chemical peel is generally manageable, but the Miami climate introduces specific variables that patients elsewhere do not face. In the first 24 to 48 hours, most patients experience mild redness and some tightness. By day 2 to 4, light peeling begins, starting around the mouth and nose where the skin is thinnest. This is normal and should not be accelerated by picking or exfoliating. By the end of week one, the majority of patients have clear, noticeably brighter skin. A peer-reviewed clinical study in the Journal of Dermatological Treatment confirming that superficial chemical peels produce measurable improvement in acne lesion counts after a standardized series supports the visible outcomes our patients consistently report.
Why humidity changes your aftercare rules
South Florida’s humidity does two things simultaneously. It helps the skin retain moisture during healing, which is beneficial. It also creates a warm, moist environment where bacteria thrive. For post-peel skin, where the surface barrier is temporarily compromised, bacterial contamination is a real risk if the skin is not kept clean and hands-off. Specific instructions we give our Doral and Miami patients:
- No sun exposure for 7 days minimum: use mineral sunscreen SPF 30 or higher every morning, regardless of whether you plan to be outside.
- Mineral sunscreen only: chemical UV filters can penetrate more readily into compromised skin and cause irritation post-peel.
- No sweating: skip outdoor workouts, beach activities, and high-humidity environments for the first week.
- Keep it clean and simple: gentle cleanser, moisturizer, sunscreen. Nothing active (no retinoids, no exfoliants) until your provider clears it.
- Hands off: do not pick the peeling skin. Premature removal of peeling skin delays healing and increases the risk of scarring.
What Makes a Medical Clinic Peel Different From a Spa Treatment
The difference between a medical peel and a spa peel is not the marketing language or the ambiance. It is the acid concentration, the pre-treatment assessment, and the clinical judgment about when not to proceed. Estheticians at spas are generally limited to lower-percentage acids by their licensure, which means the treatments are milder and the outcomes more gradual. That is not inherently a problem for maintenance, but for patients dealing with active acne, resistant hyperpigmentation, or post-inflammatory scarring, those concentrations often fall short of what the skin needs.
At Perfect B, our providers use medical-grade acid concentrations, properly prepare the skin before treatment, and assess every patient for contraindications before applying anything. The Fitzpatrick evaluation, the acne status review, the medication history check: these are not administrative steps. They are the clinical decisions that determine whether your peel helps or hurts. And critically, a medical provider knows when to say no to a treatment that a spa might offer regardless. → Explore Perfect B’s acne scars treatment plan in Doral, FL for patients ready to address the marks acne leaves behind.

Frequently Asked Questions
1. Can a chemical peel make acne worse before it gets better?
It can, in a limited way. Some patients experience a brief purging phase after their first one to two peels, where existing congestion that was below the surface gets accelerated to the surface and clears as a breakout. This typically resolves within one to two weeks and is different from a true adverse reaction. If new breakouts persist beyond the second week after treatment, contact your provider. Purging is a normal cellular turnover event. A true flare triggered by the wrong peel type or inappropriate protocol is not.
2. How soon after a chemical peel will I see results for acne?
Most patients notice brighter, smoother skin and reduced congestion within five to seven days of their first peel, once the initial shedding phase is complete. Significant acne reduction requires a series. By the third session, patients with mild to moderate acne typically see a meaningful reduction in active breakouts. By the fourth and fifth sessions, the cumulative improvement in texture, tone, and lesion frequency is substantially more pronounced than after a single treatment.
3. Is a chemical peel safe for dark skin tones?
Yes, when performed correctly by a provider who understands Fitzpatrick classification and adjusts the protocol accordingly. Superficial peels using mandelic acid or lactic acid are well tolerated on Fitzpatrick III to V skin. The risk of post-inflammatory hyperpigmentation increases with deeper peels, higher acid concentrations, and inadequate pre-treatment assessment. At our clinic in Doral, FL, Fitzpatrick assessment is a standard first step in our peel protocol.
4. Can I get a chemical peel if I have hormonal acne?
Chemical peels address surface-level acne: congestion, excess oil, dead cell accumulation, and post-inflammatory pigmentation. They do not regulate the hormonal signals that drive hormonal acne. For patients with a predominantly hormonal pattern, peels work best as one component of a broader treatment plan that addresses the hormonal trigger. A peel series will reduce surface breakouts and improve skin quality, but if the underlying hormonal dysregulation is not addressed, new breakouts will continue.
5. How long do I need to stay out of the sun after a chemical peel?
A minimum of seven days with strict sun avoidance and daily mineral sunscreen. In Miami, where UV exposure is intense year-round, we extend this guidance: wear SPF 30 or higher every morning for the two to three weeks following a peel, even on overcast days. The newly resurfaced skin has reduced melanin protection and is significantly more susceptible to UV-induced pigmentation damage. One unprotected afternoon outside can trigger hyperpigmentation that takes months to fade.
6. How much does a chemical peel cost at Perfect B in Doral?
Pricing varies based on the acid type, depth, and any adjunct treatments included in the session. We offer single-session pricing and package rates for the recommended 4-to-6 session series. Series pricing provides a meaningful discount compared to individual sessions and is what we recommend for patients pursuing acne control rather than maintenance. Contact us at (786) 502-2260 or visit our clinic in Doral for a consultation where we can review your skin and provide a specific protocol recommendation and pricing.
7. Can chemical peels be combined with other acne treatments?
Yes, and in most cases, combination approaches produce better outcomes than peels alone. At Perfect B, we commonly combine peel series with topical depigmenting agents for PIH, LED light therapy to address bacterial load between sessions, and medical-grade skincare to support barrier function during the treatment period. Peels are a powerful tool in an acne management protocol, but they work best as part of a comprehensive plan rather than a standalone solution.
Closing: The Clinical Bottom Line on Chemical Peels for Acne
Chemical peels are one of the most effective tools in acne management when they are matched correctly to the patient. The acid type has to fit the acne type. The depth has to respect the skin tone and the inflammation status. The series has to be long enough to produce cumulative change. When those variables are aligned, the results are real and measurable: clearer pores, fewer active lesions, improved texture, and significantly reduced post-acne pigmentation. When they are mismatched, the result is more damage on top of a problem that already exists.
What separates Perfect B from a spa or a retail peel experience is the clinical assessment that happens before any acid touches the skin. We evaluate Fitzpatrick type, review your current medications, assess the activity level of your acne, and make a decision about whether a peel is appropriate at all. That decision-making is not a formality. It is the treatment. → See how Perfect B’s skin rejuvenation treatment plan in Doral, FL combines chemical peels with RF microneedling, laser, and medical-grade skincare for comprehensive skin resurfacing.
📍 Visit us at Perfect B, Doral FL
📞 Call or message us at (786) 502-2260


