
Perfect B, Doral Fl. | 06.23.26 | 11 min read.
This article is for educational purposes only and does not constitute medical advice. Peptide therapy requires evaluation and prescription by a licensed medical provider. Do not use this information to self-administer or self-diagnose. Contact Perfect B at (786) 502-2260 to schedule a clinical evaluation.
What Are Peptides for Testosterone and What They Actually Do
Search volume for peptides for testosterone has roughly tripled in twelve months, climbing from about 2,900 monthly searches in mid 2025 to over 8,100 in May 2026. The interest is clear, but most of what is published online conflates two very different things: peptides that act on the growth hormone axis (CJC-1295, Ipamorelin, Tesamorelin) and peptides that act directly on the gonadal axis (Kisspeptin, Gonadorelin, HCG). The clinical reality is that peptides for testosterone do not replace testosterone, do not function as TRT, and do not directly raise serum total T in the way an injection of testosterone cypionate does. What they do, when prescribed correctly, is restore the hormonal environment in which the body’s own testosterone production works the way it did a decade earlier.
At our clinic in Doral, FL, the most common scenario is a man between 38 and 55 who has rising visceral fat, lighter sleep, slower workout recovery, and a sense that his energy and body composition have shifted in a way his habits no longer explain. Total testosterone may still be inside the lab reference range, but the downstream symptoms are real. This post is written for that patient. It covers which peptides influence testosterone, how the mechanism actually works, where peptides fit alongside TRT, and how Perfect B decides which protocol to recommend.

Not Sure Whether Peptides, TRT, or Both Fit Your Profile? See What Patients With Similar Labs Are Running at Perfect B.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
Key Takeaways
- Peptides for testosterone are not TRT: they do not replace testosterone. They restore the upstream hormonal environment (growth hormone, IGF-1, body composition) in which your own testosterone functions more efficiently.
- Two separate pathways exist: the growth hormone axis (CJC-1295, Ipamorelin, Tesamorelin) and the gonadal axis (Kisspeptin, Gonadorelin). Perfect B prescribes growth hormone axis peptides because of their safety profile and durable body composition effects.
- Clinically low testosterone needs TRT: if your total testosterone is well below range with broad symptoms, peptides alone will not correct that. The honest clinical answer is TRT, sometimes with peptides used alongside.
- Visceral fat is the central variable: excess visceral fat suppresses testosterone and increases aromatization to estrogen. Tesamorelin and CJC-1295 / Ipamorelin both reduce visceral fat under supervision, and that change alone can shift hormonal output.
- Supervision is non-negotiable: every peptide protocol at Perfect B begins with a licensed provider intake, baseline labs (testosterone, free T, estradiol, IGF-1, fasting glucose, lipid panel), and an InBody scan to quantify visceral fat and lean mass before prescribing.
The Two Hormonal Pathways Behind Peptides for Testosterone
The phrase peptides for testosterone gets used as if it described a single category, but it does not. Two completely different sets of peptides get marketed under that label, and they act on different parts of the endocrine system. Understanding the distinction is the difference between a protocol that delivers durable change and one that does nothing useful.
The Growth Hormone / IGF-1 Axis (Indirect)
Peptides like CJC-1295, Ipamorelin, and Tesamorelin act on the hypothalamic pituitary axis. They signal the pituitary gland to release the patient’s own growth hormone, which in turn triggers the liver to produce IGF-1 (insulin-like growth factor 1). The downstream effects include deeper sleep, faster recovery, improved insulin sensitivity, reduced visceral fat, and increased lean mass. Each one of those changes feeds back into testosterone production indirectly. Less visceral fat means less aromatase activity, which means less conversion of testosterone to estrogen. Better sleep restores the overnight luteinizing hormone (LH) pulses that drive testicular testosterone synthesis. Improved insulin sensitivity reduces the metabolic stress that suppresses the gonadal axis. None of these peptides raise testosterone directly, but the cumulative effect of restoring the upstream environment is measurable in patients we see in Miami.
The Gonadal Axis (Direct)
A separate group of peptides, Kisspeptin, Gonadorelin, and HCG, acts directly on the hypothalamic pituitary gonadal axis. Kisspeptin stimulates GnRH release from the hypothalamus. Gonadorelin is a synthetic GnRH analog. HCG mimics luteinizing hormone at the testicular level. These compounds can raise testosterone directly because they trigger the testes to produce more of it. The reason Perfect B does not include them in our standard peptide menu is that the safety, dosing, and monitoring requirements are different from the growth hormone axis peptides, and the use cases (fertility preservation during TRT, post-cycle therapy, hypothalamic dysfunction) are narrower than what most men searching this term actually need.

Why Perfect B Uses the Growth Hormone Pathway Specifically
The choice to focus on the growth hormone axis rather than the gonadal axis is deliberate. It comes down to four clinical factors: safety profile, the patient population we see in Doral, the durability of results, and the ability to combine cleanly with TRT when both are appropriate.
- Safety profile: CJC-1295, Ipamorelin, and Tesamorelin have well-documented mechanisms and decades of human data behind them. Tesamorelin is FDA-approved for visceral fat reduction in HIV-associated lipodystrophy, with a 26-week pivotal trial published in the New England Journal of Medicine. Ipamorelin is documented as selective for growth hormone release without elevating cortisol or prolactin, which is a problem with older secretagogues like GHRP-6.
- The Miami patient profile: the majority of men in their 40s and 50s we see do not have primary hypogonadism. They have visceral fat accumulation, metabolic syndrome features, and lifestyle-driven hormonal decline. Treating the visceral fat and the GH axis often resolves the symptoms that brought them in.
- Durability: the body composition changes from growth hormone axis peptides persist after appropriate cycling. The gains in lean mass and reductions in visceral fat do not vanish the day the protocol ends, which is different from how the gonadal axis peptides behave when discontinued.
- Compatibility with TRT: for men who do need TRT, growth hormone axis peptides combine cleanly with testosterone replacement and address the things TRT alone does not (sleep architecture, visceral fat, IGF-1, recovery). This is a common combined protocol in our practice.
Peptides vs TRT: What They Actually Do Differently
This is the most common question we get and the most commonly misunderstood. TRT replaces testosterone. Peptides do not. They are not interchangeable, they are not alternatives in the strict sense, and the right answer often depends on what the labs and the InBody scan actually show.
When TRT Is the Right Answer
If your total testosterone is well below the reference range, your free T is low, and you have broad symptoms (fatigue, low libido, erectile changes, mood, loss of muscle), TRT is going to do what peptides cannot. It directly elevates circulating testosterone, often with noticeable changes inside two to three weeks. The tradeoffs are well known: testicular suppression, potential fertility impact, possible red blood cell increases, and the long-term commitment that comes with hormone replacement.
When Peptides Are the Right Answer
If your testosterone is borderline or in the low-normal range, your visceral fat is elevated, your sleep has degraded, and your symptoms are concentrated around recovery, body composition, and energy, growth hormone axis peptides are often the right starting point. They do not commit you to lifelong hormone replacement, they do not suppress endogenous testicular function, and the upstream improvements they produce often resolve the symptoms that initially looked like low testosterone.
When Both Together Is the Answer
For a meaningful subset of men in their 40s and 50s, TRT alone improves total T but does not fully restore sleep, visceral fat, or recovery to baseline. Adding a growth hormone axis peptide to an existing TRT protocol addresses those specific gaps. The combined approach is one of the most common protocols we run at our Doral clinic for men who have already been on TRT for a year or more and are looking to recover the rest of what they were promised.
Not sure whether peptides, TRT, or both fit your profile?
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
The Three Peptides Perfect B Uses for Male Hormonal Health
The growth hormone axis peptides we prescribe at our Doral clinic fall into three categories, each suited to a different clinical profile.
Tesamorelin: For Visceral Fat Driven Hormonal Decline
Tesamorelin is a synthetic analog of growth hormone releasing hormone (GHRH) with one of the strongest peer-reviewed safety records among peptides. It binds GHRH receptors at the pituitary, triggers a physiologic pulse of growth hormone, and produces measurable reductions in visceral adipose tissue within 12 to 26 weeks. A 2010 New England Journal of Medicine pivotal trial by Falutz et al. demonstrating that tesamorelin reduced visceral adipose tissue by a mean of 18 percent over 26 weeks compared to placebo in patients with abdominal fat accumulation remains the foundational evidence behind its clinical use. For men whose central problem is visceral fat and the metabolic and hormonal cascade that follows from it, Tesamorelin is the first choice. We explain the mechanism in depth in our complete clinical guide to Tesamorelin and how it works at the cellular level.
CJC-1295 / Ipamorelin: For Lean Mass, Sleep, and Recovery
CJC-1295 and Ipamorelin are prescribed together as the most common peptide stack at our clinic. CJC-1295 is a GHRH analog with an extended half-life. Ipamorelin is a selective growth hormone secretagogue that binds the ghrelin receptor in the pituitary. The combination triggers a larger, cleaner growth hormone pulse than either compound alone, with a side effect profile that does not include the cortisol or prolactin elevations seen with older secretagogues. For men whose central concern is sleep architecture, recovery between training, and lean mass preservation rather than visceral fat per se, CJC-1295 / Ipamorelin is the preferred protocol. The mechanism is broken down in our full clinical breakdown of what CJC-1295 / Ipamorelin actually is and why it works the way it does.
Wolverine Stack (BPC-157 + TB-500): For Recovery and Tissue Repair
The Wolverine stack is not a testosterone peptide per se, but it appears in many of our male protocols for men in their 40s and 50s who are training seriously and recovering slowly. BPC-157 targets localized tissue repair, tendon regeneration, and gut mucosal healing. TB-500 acts systemically, regulating actin and supporting stem cell mobilization. The two together produce faster and higher-quality recovery than either alone. For an active patient whose primary frustration is that recovery has stopped keeping up with training, the Wolverine stack is often layered onto the growth hormone protocol. Our full guide to the Wolverine peptide stack covering BPC-157 and TB-500 mechanisms and the synergistic healing pathways covers when and why we prescribe it.
How We Decide Which Peptide for Which Patient at Perfect B
This is the part of the conversation that almost no online article gets right. The choice between Tesamorelin, CJC-1295 / Ipamorelin, the Wolverine stack, TRT, or a combination is not a preference. It is a clinical decision based on objective measurements from a baseline workup.
- Baseline labs: total testosterone, free testosterone, estradiol, SHBG, LH, FSH, IGF-1, fasting glucose, HbA1c, lipid panel, complete blood count, and PSA when age-appropriate. These tell us where the hormonal axis is and what is suppressing what.
- InBody scan: we use this body composition measurement to quantify visceral fat, skeletal muscle mass, and segmental composition before deciding which peptide to prescribe. A patient with elevated visceral fat and otherwise normal muscle mass is a Tesamorelin candidate. A patient with low skeletal muscle and normal visceral fat is a CJC-1295 / Ipamorelin candidate. A patient with both is often prescribed a layered protocol.
- Symptom mapping: we map the patient’s symptoms (sleep, recovery, libido, energy, mood) against the lab and InBody data. A man with broad symptoms and clinically low testosterone is referred for TRT evaluation. A man with focal symptoms and borderline labs is started on peptides first.
- Lifestyle factors: alcohol intake, sleep duration, training load, and nutrition all blunt or amplify peptide response. We discuss these openly with the patient at intake because the protocol does not work in isolation from the rest of the life around it.
What Men in Their 40s and 50s at Our Doral Clinic Notice First
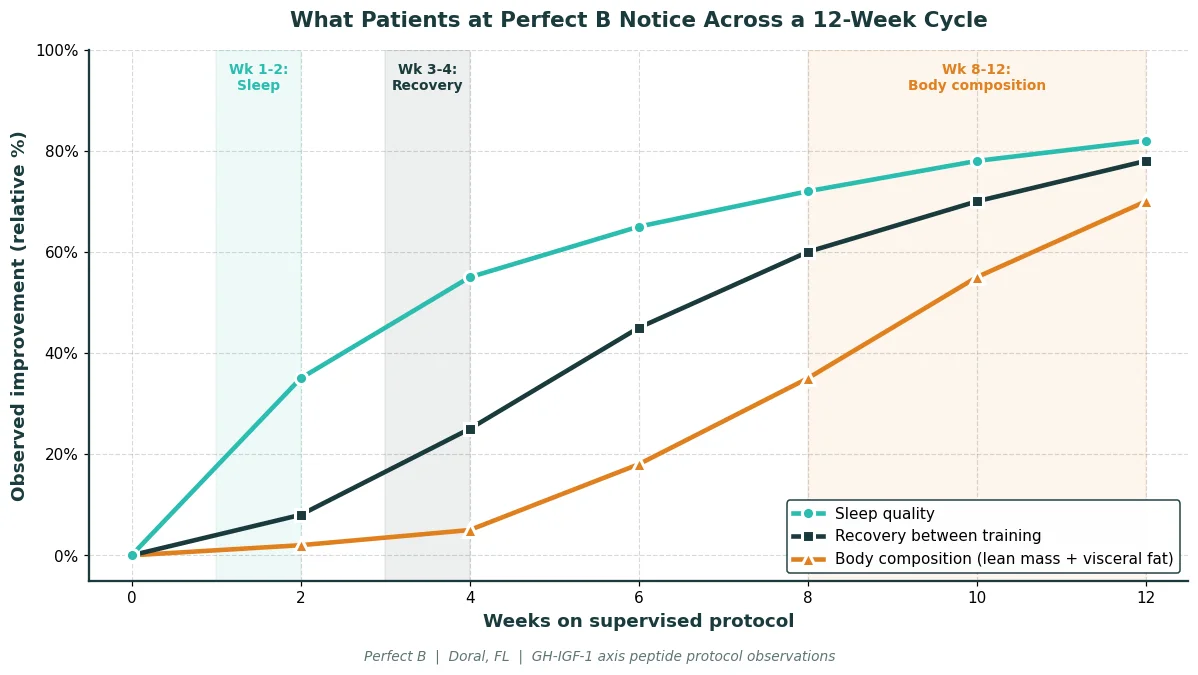
The timeline of what patients report on a supervised growth hormone axis peptide protocol is remarkably consistent. Exact timing varies with age, baseline body composition, training load, and sleep quality, but the sequence of changes follows a predictable pattern across a 12-week cycle.
- Weeks 1 to 2: sleep quality is the first change most patients report. Falling asleep faster, sleeping more deeply, and waking with more energy than they had the morning before. This is the earliest and most universal sign the protocol is working.
- Weeks 3 to 4: recovery between training sessions shortens. Workouts that used to require two days to recover from start to turn over in one. Patients training regularly report this with unusual consistency.
- Weeks 4 to 8: body composition begins to visibly shift. Lean mass fills out, the midsection tightens, and the InBody scan starts to show measurable reductions in visceral fat. Men who had plateaued in a weight loss or training protocol commonly break through during this window.
- Weeks 8 to 12: energy becomes more consistent across the day. Skin tone and sometimes hair quality improve. Repeat labs at this point often show IGF-1 trending into the upper third of the age-adjusted range, with estradiol and SHBG shifting in patterns that suggest improved overall hormonal regulation.
What Peptides for Testosterone Will Not Do
Honesty about what these compounds cannot do is part of the conversation. The marketing language that treats peptides as a one-for-one testosterone replacement is wrong, and most of the disappointment we see in patients who came to us after self-administering peptides bought online comes from believing the marketing.
- They will not replace clinically low testosterone: if your total T is well below range and the symptoms are broad, peptides alone will not correct that. The honest answer is TRT, with peptides considered as an adjunct.
- They will not work overnight: the timeline is weeks to months, not days. Patients looking for a fast spike will not get one with growth hormone axis peptides.
- They will not overcome poor sleep, heavy alcohol intake, or no training: the protocol is a multiplier. If the inputs are not there, the multiplier has nothing to work with. We address this directly at intake because a protocol that gets undermined by lifestyle factors is a protocol that does not work.
- They will not safely run without supervision: peptides bought online without labs, without provider oversight, and without injection technique training are how patients end up with injection site infections, glucose dysregulation, or no results at all. The compounding pharmacy, the labs, the dosing decisions, and the cycling protocol are not optional.
Peptides for Testosterone Treatment Plan at Perfect B
The peptide treatment plan at our Doral clinic begins with a consultation that covers symptoms, history, and treatment goals. Baseline labs and the InBody scan happen at that visit or shortly after. The protocol that follows is built around the data, not chosen from a menu.
Cycles typically run on a structured schedule with defined pauses. Reconstitution, injection technique, storage, and rotation are taught in person before the patient leaves with their first vial. Repeat labs and an InBody comparison at the end of the cycle determine whether to continue, adjust, or change peptide entirely. Payment options at Perfect B include Cherry, Klarna, Afterpay, and CareCredit so the protocol does not get derailed by the cost of a single vial. The full treatment plan structure is on our medical peptide treatment plan page covering the full clinical protocol Perfect B uses at our Doral clinic.

See What Patients With Similar Goals Are Running at Perfect B in Doral.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
Frequently Asked Questions
1. Do peptides actually raise testosterone?
Growth hormone axis peptides like CJC-1295, Ipamorelin, and Tesamorelin do not raise serum total testosterone directly. They reduce visceral fat, improve sleep architecture, and restore IGF-1, all of which create a hormonal environment in which the body’s own testosterone production functions more efficiently. Direct increases in measured T from these peptides are inconsistent in the literature. The clinical benefit is real, but it is downstream rather than direct. The gonadal axis peptides (Kisspeptin, Gonadorelin, HCG) can raise testosterone more directly, but they are not part of the standard menu at Perfect B for reasons explained earlier in this article.
2. What is better, TRT or peptides?
That depends on what the labs show. If total testosterone is clearly low (well below the reference range) and the symptoms are broad, TRT is going to do what peptides cannot. If testosterone is borderline or in the low-normal range and the central problem is visceral fat, sleep, and recovery, growth hormone axis peptides are often the better starting point. For a meaningful subset of patients, the right answer is both together. The decision is made at intake with labs and InBody data, not by preference or marketing.
3. Can peptides for testosterone be used alongside TRT?
Yes, and it is one of the most common combined protocols in our practice. TRT replaces the testosterone. Growth hormone axis peptides address the things TRT alone does not, especially sleep architecture, visceral fat, IGF-1, and recovery. Men who have been on TRT for a year or more often come to us because they got the testosterone correction but not the rest, and adding a peptide protocol fills in those gaps. The combined protocol is managed by the same provider with coordinated labs.
4. What are the best peptides for men over 40?
For men in their 40s and 50s, the three growth hormone axis peptides that consistently produce results at our Doral clinic are Tesamorelin (for patients whose central problem is visceral fat), CJC-1295 / Ipamorelin (for sleep, recovery, and lean mass), and the Wolverine stack of BPC-157 and TB-500 (for recovery and tissue repair when training load is the limiting factor). The right choice depends on the InBody scan and the symptom pattern, not on age alone.
5. How long does it take for peptides for testosterone to work?
Sleep typically changes inside 1 to 2 weeks. Recovery improvements show up in weeks 3 to 4. Visible body composition changes start around week 4 to 8 and continue building through week 12. Repeat labs at the end of the first cycle commonly show IGF-1 trending into the upper third of the age-adjusted range. Patients expecting a faster timeline are usually thinking about TRT timelines, not peptide timelines.
6. Are peptides for testosterone safe?
Under supervision, with compounding pharmacy quality, baseline and follow-up labs, and a defined cycling protocol, the peptides Perfect B prescribes have well-documented safety profiles. The risk is not in the peptide itself when used correctly. The risk is in unsupervised online sources, unverified compounding, no labs, and no provider oversight. The injection site infections, glucose dysregulation, and lack of results we see in patients who came in after self-administering all trace back to the absence of those four pillars.
7. Can peptides cause infertility like TRT can?
Growth hormone axis peptides (CJC-1295, Ipamorelin, Tesamorelin) do not suppress testicular function and do not impact fertility the way TRT can. This is one of the reasons younger men with borderline testosterone who want to preserve fertility are often started on the peptide pathway rather than committed to TRT. The gonadal axis peptides have different fertility implications and are used specifically in fertility preservation contexts under appropriate specialty care.
Closing: The Clinical Bottom Line on Peptides and Testosterone
Peptides for testosterone are not what most online sources claim. They are not TRT. They do not raise serum T directly in a way that resolves clinically low testosterone. What they do, when prescribed correctly on the growth hormone axis, is restore the upstream environment (sleep, visceral fat, IGF-1, recovery) in which the body’s own testosterone production works more efficiently. For the patient who is borderline rather than clinically low, that upstream restoration is often enough to resolve what brought him to the clinic. For the patient who is clinically low, peptides are an adjunct to TRT, not a substitute. The honest version of the conversation is the one that starts with labs and an InBody scan, not with a peptide name.
The difference between a supervised protocol at Perfect B and a vial purchased from an online source is not the peptide. It is the labs, the dosing decisions, the cycling protocol, the compounding pharmacy quality, and the provider who reviews how the body is actually responding. That is the part that makes the difference between a protocol that works and one that does not. South Florida patients can reach Perfect B at our Doral location to schedule a clinical evaluation and review whether peptides, TRT, or both fit their specific labs and goals.
- 📍 Visit us at Perfect B | 3905 NW 107th Ave, Suite 104, Doral FL 33178
- 📞 Call or message us at (786) 502-2260
- 💳 Buy Now Pay Later available: Cherry, Klarna, Afterpay, CareCredit
→ Book your peptide consultation at Perfect B in Doral today.


