
Perfect B, Doral Fl. | 06.23.26 | 10 min read.
This article is for educational purposes only and does not constitute medical advice. Peptide therapy requires evaluation and prescription by a licensed medical provider. Do not use this information to self-administer or self-diagnose. Contact Perfect B at (786) 502-2260 to schedule a clinical evaluation.
What Peptides for Women Over 40 Actually Are
Search interest in peptides for women over 40 has grown almost ten times in twelve months, from about 90 monthly searches in mid 2025 to nearly 880 in May 2026. The interest is real because the biological shift it points to is real. Peptides are short chains of amino acids that act as signaling molecules, telling specific cells to repair tissue, release growth hormone, support metabolism, or rebuild collagen. For women in the 40s who are noticing slower recovery, body composition changes, lighter sleep, or thinning skin even though their habits have not changed, the appeal is that peptides target a specific biological mechanism rather than offering a blunt, one-size-fits-all fix.
The challenge is that most of what is published online comes from supplement sellers or clinics pushing whatever peptide they happen to stock. This post is the version a medical clinic in Doral, FL would write. It covers what peptides are actually appropriate for women over 40, what has to be in place before they make sense, how Perfect B decides which peptide for which patient, and where peptides fit alongside hormone therapy rather than instead of it.

Not Sure Which Peptide Protocol Fits Your Goals? See What Women Patients Over 40 Are Running at Perfect B.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
Key Takeaways
- Peptides are chosen by goal, not by stack: skin, body composition, recovery, fat metabolism, and energy each have different peptides behind them. There is no single best peptide for women over 40.
- The biological shift starts at 35, not at menopause: growth hormone production declines from the mid-30s, regulated by the early estrogen shifts of perimenopause, often a decade before menopause arrives.
- Foundation first, peptides second: nutrition, strength training, sleep, and hormonal evaluation come before any peptide decision. Peptides amplify a working system, they do not compensate for a broken one.
- Peptides do not replace hormone therapy: for women in perimenopause and menopause, peptides support sleep, body composition, and recovery alongside hormone therapy when appropriate, not instead of it.
- InBody scan plus labs guide the protocol: at Perfect B in Doral, body composition data combined with hormonal labs determines which peptide and at what point in a woman’s clinical picture it makes sense.
Why the Biological Shift Starts at 35, Not at Menopause
Growth hormone in women is not a steady background signal. It pulses, primarily during deep sleep, and those pulses are regulated in part by estrogen. When estrogen begins its gradual perimenopause transition in the mid-to-late 30s, GH pulse amplitude and frequency decline alongside it. Women in the Miami area often notice the downstream effects years before connecting them to growth hormone: sleep becomes lighter, recovery from exercise takes longer, body fat shifts toward the abdomen, and skin begins losing density.
The clinical literature confirms that women have higher baseline GH secretion than men during the reproductive years, partly because estrogen stimulates GH release from the pituitary. This higher baseline is protective. When it starts to drop, the change is not gradual across decades. It is a measurable shift that correlates with perimenopause onset, not with menopause itself. By the time a woman reaches full menopause, she has already been losing GH pulse frequency for 10 to 15 years.
Perimenopause Is the Inflection Point, Not Menopause
A woman who feels that her body has changed after 35 without a clear explanation is often correct, and the GH axis is one of the primary reasons. The fatigue is real. The change in body composition is real. Waiting for a menopause diagnosis before addressing it means waiting through the years when intervention is most effective. We cover this in clinical depth in our clinical breakdown of why the growth hormone axis changes after 35 in women and what to do about it.
The Symptoms Women in Their 40s Notice First
Across patients we see at our Doral clinic, the early signs cluster in a predictable pattern. Sleep becomes lighter and less restorative, often with waking around 3 or 4 AM. Body composition shifts toward more abdominal fat and less lean mass, even when nutrition and training have not changed. Workouts that used to require one recovery day now require two. Skin loses some of its bounce and elasticity. None of these is dramatic in isolation. Together they form the pattern most women describe as “something has shifted.”
What Has to Be in Place Before Peptides Make Sense
This is the part of the conversation most online sources skip. Peptides do not work in a vacuum. They amplify the signal in a system that is already functioning. At Perfect B in Doral, the prerequisites that come before any peptide decision are not optional.
- Baseline labs: a comprehensive hormonal and metabolic panel including estradiol, progesterone, testosterone, thyroid function, IGF-1, fasting glucose, HbA1c, and lipid panel. These tell us where the hormonal axis currently is and what is influencing it.
- InBody body composition scan: we use this measurement to quantify visceral fat, skeletal muscle mass, and segmental composition before deciding which peptide to prescribe. The numbers from this scan directly inform the protocol.
- Hormonal evaluation: if a woman is in perimenopause or menopause, the question of whether she needs hormone therapy is addressed first or alongside the peptide decision. Peptides are not a substitute for the foundational hormonal restoration that hormone therapy provides when indicated.
- Nutrition and strength training: protein adequacy and consistent strength training are central, not optional. Lean mass preservation is the single most important variable for body composition outcomes in women over 40, and no peptide will compensate for an absence of strength training.
- Sleep: growth hormone peptides work primarily during deep sleep. A woman sleeping four broken hours a night will see less response than one sleeping seven consistent hours. Sleep optimization is part of the protocol, not an afterthought.
Only when these foundations are addressed does the conversation about peptides start. This is not a stalling tactic. It is the difference between a protocol that produces measurable change and one that produces frustration.
The Peptides Perfect B Prescribes for Women Over 40, Organized by Goal
There is no single best peptide for women over 40. The right choice depends on what a patient is trying to change. The catalog below reflects what we actually prescribe at our Doral clinic, grouped by the goal each peptide serves. For a broader view of how each of these fits across women of different ages and goals, see our complete clinical guide to the best peptides for women organized by goal.
Skin, Collagen, and Visible Aging: GHK-Cu
GHK-Cu is a copper peptide with one of the strongest research records in skin biology. It supports collagen and elastin production and helps the skin repair its barrier, which is why it is often the first peptide women over 40 ask about when their goal is firmer, healthier skin. A peer-reviewed clinical trial in the Journal of Aging Science showing that topical GHK-Cu reduced wrinkle volume by 55.8 percent in women aged 40 to 65 over 8 weeks remains one of the cleaner human data sets on copper peptides. GHK-Cu pairs naturally with in-clinic skin treatments rather than competing with them.
Body Composition, Sleep, and Energy: CJC-1295 with Ipamorelin
The CJC-1295 with Ipamorelin combination is the most requested growth hormone peptide stack at our clinic. CJC-1295 is a GHRH analog with an extended half-life. Ipamorelin is a selective growth hormone secretagogue that binds the ghrelin receptor in the pituitary. The combination prompts the body to release its own growth hormone in a more natural rhythm, which patients connect with deeper sleep, improved recovery, and gradual changes in lean mass and body composition. It is not a shortcut, and results build over weeks rather than days.
Recovery, Joints, and Tissue Repair: Wolverine Stack (BPC-157 with TB-500)
The Wolverine stack combines BPC-157 and TB-500, two peptides that work through complementary tissue repair mechanisms. BPC-157 targets localized tissue healing, tendon regeneration, and gut mucosal integrity. TB-500 acts systemically, supporting cellular migration and stem cell mobilization. Together they produce faster, higher-quality recovery than either alone. For women over 40 dealing with tendon strain, joint discomfort, or the slower recovery that comes with declining GH, the Wolverine stack is often layered onto a growth hormone protocol.
Visceral Fat and Metabolic Stall: Tesamorelin
Tesamorelin is a synthetic analog of growth hormone releasing hormone (GHRH) with one of the strongest peer-reviewed safety records among peptides. It is FDA-approved for visceral fat reduction in HIV-associated lipodystrophy, with a 26-week pivotal trial published in the New England Journal of Medicine. For women over 40 whose body composition has stalled despite consistent effort, particularly with visceral fat accumulation in the midsection, Tesamorelin is the targeted option. We explain the mechanism in depth in our complete clinical guide to Tesamorelin peptide and how it works at the cellular level.
Cellular Energy and Metabolism: MOTS-c
MOTS-c is a mitochondrial-derived peptide studied for its role in metabolism, insulin sensitivity, and cellular energy production. Women who describe persistent fatigue and a sense that their metabolism has slowed, often despite normal labs and adequate sleep, are sometimes candidates for MOTS-c as part of a broader metabolic protocol. As with the others, the honest framing is supportive, not miraculous. MOTS-c works best when nutrition and training are already in place.
How Perfect B Decides Which Peptide for Which Patient
This is the part of the conversation almost no online article gets right. The choice between GHK-Cu, CJC-1295 with Ipamorelin, the Wolverine stack, Tesamorelin, or MOTS-c is not a preference. It is a clinical decision based on objective measurements from a baseline workup.
- InBody scan results: a patient with elevated visceral fat and otherwise normal muscle mass is a Tesamorelin candidate. A patient with low skeletal muscle and normal visceral fat is a CJC-1295 with Ipamorelin candidate. A patient with both visceral fat accumulation and low skeletal muscle is often prescribed a layered protocol combining the two.
- Lab data: IGF-1 baseline tells us where on the GH decline curve a patient currently sits. Estradiol and hormonal panel results determine whether hormone therapy is the primary intervention with peptides as adjunct, or whether peptides are the standalone path.
- Symptom mapping: we map the patient’s symptoms (sleep quality, recovery, skin, body composition, energy) against the lab and InBody data. A woman whose primary concern is skin is started differently than a woman whose primary concern is visceral fat or recovery.
- Lifestyle factors: training load, sleep quality, alcohol intake, and nutrition all change peptide response. We discuss these openly at intake because a protocol that gets undermined by lifestyle factors is a protocol that will not produce the result the patient expected.
Peptides and Hormone Replacement Therapy: Complementary, Not Competitive
One of the most common misconceptions is that peptides are an alternative to hormone replacement therapy. They are not. Peptides for women over 40 are used to support sleep, body composition, recovery, and skin. They do not replace hormone therapy when hormone therapy is what a patient actually needs.
For women in perimenopause and menopause with significant symptoms (vasomotor symptoms, sleep disruption tied to hormonal shifts, mood, vaginal changes, bone density concerns), hormone therapy is the foundational intervention. Peptides can layer on top of hormone therapy to address what hormones alone do not fully restore, such as body composition shifts that persist despite hormonal restoration, or the recovery and skin changes tied to declining growth hormone. For context on how this works at the biological level, see a National Library of Medicine review examining estrogens and neuropeptide signaling in postmenopausal women.
The two work through different mechanisms. Hormone therapy restores foundational hormone levels. Peptides work at the level of cellular signaling, growth hormone release, and tissue repair. They are complementary, not competing. At our Doral clinic, many of our best patient outcomes involve a combined protocol of hormone therapy and targeted peptides matched to the patient’s labs and goals.
See How Peptides Fit Into a Supervised Protocol for Women Over 40 at Perfect B.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
What Women in Their 40s at Our Doral Clinic Notice First
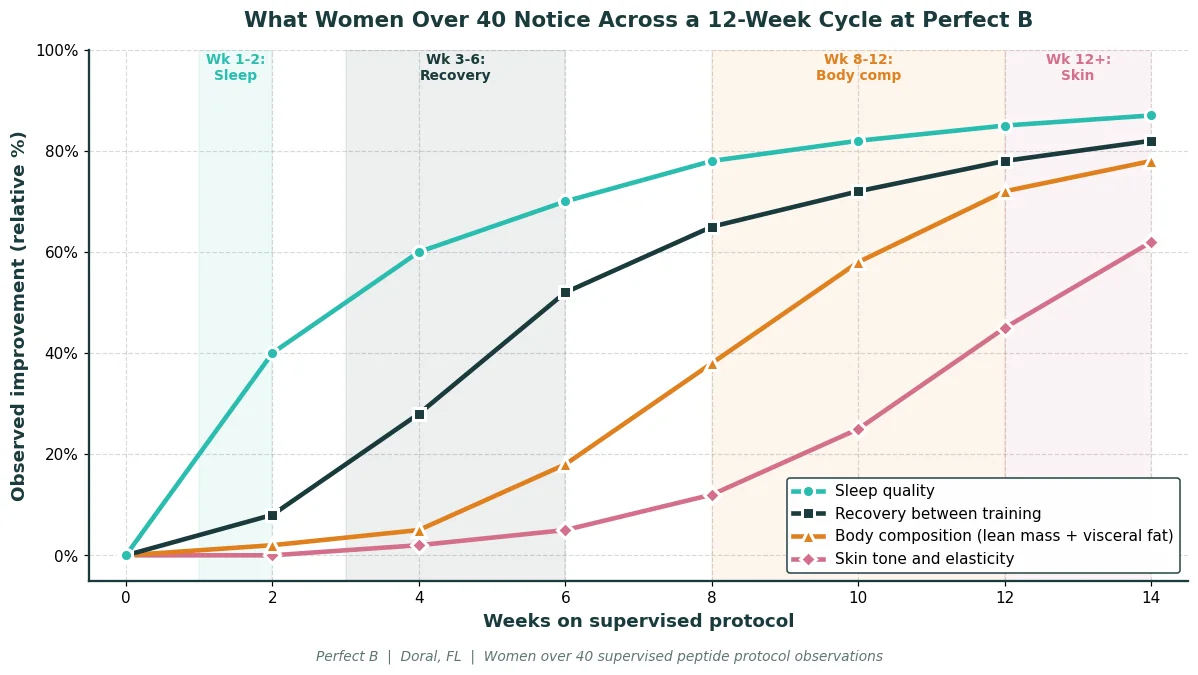
The timeline of what patients report on a supervised peptide protocol is remarkably consistent. Exact timing varies with age, baseline body composition, sleep quality, training load, and whether hormone therapy is part of the picture. But the sequence of changes follows a predictable pattern across a 12-week cycle.
- Weeks 1 to 2: sleep quality is the first change most women report. Falling asleep faster, sleeping more deeply, and waking with more energy than they had the morning before. For growth hormone axis peptides, this is the earliest and most universal sign the protocol is working.
- Weeks 3 to 6: recovery between workouts improves and morning stiffness reduces. Women training regularly report this with consistency, and it is one of the first changes that is visible to others (less midday fatigue, more energy through the afternoon).
- Weeks 8 to 12: body composition begins to visibly shift. Lean mass fills out, the midsection tightens, and the InBody scan starts to show measurable reductions in visceral fat. Women who had plateaued in a weight loss or training protocol often break through during this window.
- Weeks 12 and beyond: skin tone and elasticity improvements become noticeable. Hair quality often improves alongside, and repeat labs at this point typically show IGF-1 trending into the upper third of the age-adjusted range, with hormonal markers shifting in patterns that suggest improved overall regulation.
What Peptides for Women Over 40 Will Not Do
Honesty about what these compounds cannot do is part of the conversation. Most of the disappointment we see in patients who came to us after trying peptides on their own traces back to expectations that did not match clinical reality.
- They will not replace hormone therapy: if a woman in menopause has significant vasomotor symptoms, sleep disruption tied to hormones, or bone density concerns, peptides alone will not address those. Hormone therapy is the foundational answer, with peptides as adjunct when appropriate.
- They will not work without foundation: without strength training, protein adequacy, consistent sleep, and a functioning hormonal baseline, the peptide is a multiplier with nothing to multiply. We address this at intake because the protocol does not work in isolation.
- They will not produce immediate results: sleep changes appear inside 1 to 2 weeks, but body composition and skin changes are an 8 to 12 week timeline at minimum, often longer. Patients looking for a fast result are usually thinking about a different category of intervention.
- They will not safely run without supervision: peptides bought online without labs, without provider oversight, and without injection technique training are how women end up with injection site infections, glucose dysregulation, or no results at all. The compounding pharmacy, the labs, the dosing decisions, and the cycling protocol are not optional.
Safety and Contraindications Women Should Know
Peptides are generally well tolerated when prescribed and supervised, but they are not appropriate for everyone. Pregnancy and breastfeeding are clear reasons to wait. Women with a personal or strong family history of certain cancers, active thyroid disease, or significant hormone-sensitive conditions need careful evaluation before starting growth hormone peptides. Side effects, when they occur, tend to be mild and dose related, such as injection site irritation or temporary water retention. A responsible provider reviews medications and existing conditions before any protocol decision.
Why Supervision Makes the Difference (vs. Research Peptides Online)
This is the single most important distinction for any woman considering peptides. Much of what is sold online is labeled as research material, is not intended for human use, and carries no guarantee of purity, dosing accuracy, or sterility. A medical clinic prescribes peptides through licensed compounding pharmacies, screens health history, runs appropriate lab work, and adjusts dosing based on how the patient responds. That oversight is the product.
Peptides act on precise biological pathways, which is exactly why dose accuracy and product quality matter. The same compound at different purities or dosing strengths produces different outcomes. The difference between a supervised protocol and a vial purchased from an online source is not the peptide name. It is the labs, the dosing decisions, the cycling protocol, the compounding pharmacy quality, and the provider who reviews how the body is actually responding.
How to Start at Perfect B: Consultation, Labs, InBody Scan
A responsible start looks the same regardless of the goal. It begins with a consultation and a full history, moves to appropriate lab work and an InBody body composition scan, and ends with a protocol matched to the patient’s physiology rather than a stock stack. Most women begin with one or two targeted peptides, monitor their response over a cycle of roughly 8 to 12 weeks, and expand or adjust only if it makes sense given how they are responding.
At our clinic in Doral, FL, women over 40 most often come in for some combination of body composition, energy, sleep, and skin. The plan is built around whichever of those matters most to the patient, with the others addressed as they progress. The full treatment plan structure is on our medical peptide treatment plan page with the full Perfect B clinical protocol.

See What Women Patients With Similar Goals Are Running at Perfect B.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
Frequently Asked Questions
1. What are the best peptides for women over 40?
There is no single best peptide for women over 40. The right choice depends on the goal. GHK-Cu is favored for skin and visible aging. CJC-1295 with Ipamorelin is the most requested option for body composition, sleep, and energy. The Wolverine stack of BPC-157 with TB-500 is used for recovery, joint, and tissue repair. Tesamorelin targets visceral fat and metabolic stall. MOTS-c supports cellular energy and metabolism. The right peptide is matched to your physiology in a supervised plan based on InBody scan results, labs, and symptom mapping.
2. What is the downside of taking peptides?
The most common issues with peptides are not with the compounds themselves when prescribed and supervised. They come from unsupervised online purchases (unknown purity, incorrect dosing, no oversight) and from unrealistic expectations about timeline. Peptides take 8 to 12 weeks to produce visible body composition changes and do not work without foundational nutrition, training, and sleep. Side effects, when they occur in a supervised setting, are typically mild (injection site irritation, temporary water retention). The downsides cluster around unsupervised use, not around peptide therapy as a category.
3. What peptide is best for belly fat in women over 40?
For women over 40 whose primary concern is visceral fat (abdominal fat that builds up around organs and correlates with metabolic risk), Tesamorelin is the targeted option. It is the most peer-reviewed peptide for visceral fat reduction, originally approved for visceral fat in HIV-associated lipodystrophy. For women whose belly fat is part of a broader body composition issue with low skeletal muscle, CJC-1295 with Ipamorelin is more appropriate because it addresses overall body composition rather than just visceral fat. The InBody scan is what tells us which of these fits the specific case.
4. Are peptides good for perimenopause?
Peptides can be helpful during perimenopause to support the specific symptoms tied to declining growth hormone, including lighter sleep, slower recovery, body composition shifts, and skin changes. They are not a replacement for hormone therapy when hormone therapy is indicated for perimenopause-related symptoms. The most sensible approach is a clinical evaluation that looks at hormones, labs, and goals together, then decides whether peptides have a supporting role alongside hormone therapy or as a standalone path for the specific concerns the patient has.
5. How long do peptides take to work in women over 40?
Sleep changes typically appear inside 1 to 2 weeks. Recovery improvements show up in weeks 3 to 6. Visible body composition changes start around week 8 to 12 and continue building beyond. Skin and hair improvements become noticeable from week 12 onward. The timeline varies by peptide, by individual physiology, and by how well the foundational pieces (nutrition, training, sleep, hormonal baseline) are in place. Peptides support consistent habits, they do not replace them.
6. Can I take peptides if I am already on HRT?
Yes, and it is one of the most common protocols we run at our Doral clinic for women over 40. Hormone replacement therapy restores foundational hormone levels. Peptides work through cellular signaling, growth hormone release, and tissue repair. They are complementary, not competing. Many women on HRT add peptides to address what hormones alone do not fully restore, such as body composition changes or recovery and skin. The combined protocol is managed by the same provider with coordinated labs.
7. How does Perfect B decide which peptide is right for me?
The decision is based on baseline labs, an InBody body composition scan, and symptom mapping. The InBody scan quantifies visceral fat, skeletal muscle mass, and segmental composition. Labs cover the hormonal and metabolic baseline. Together with your symptom pattern, these tell us whether you are a candidate for GHK-Cu, CJC-1295 with Ipamorelin, the Wolverine stack, Tesamorelin, MOTS-c, or a layered protocol. The decision is clinical, not preferential.
Closing: The Clinic Takeaway on Peptides for Women Over 40
Peptides for women over 40 are not a single product or a quick fix. They are a set of targeted tools that, matched to the right goal and supervised properly, can support skin, recovery, body composition, energy, and the changes that come with perimenopause and menopause. The biological shift starts around 35, not when menopause arrives, which is why the years between 35 and 50 are when these tools are most clinically effective.
The difference between a meaningful result and a disappointing one is rarely the peptide itself. It is whether a licensed provider screened the patient, ran the labs, looked at body composition data, sourced the compound through a quality compounding pharmacy, and adjusted the dosing over time. Women in Miami or South Florida weighing peptide therapy can reach Perfect B at our Doral location to schedule a clinical evaluation that treats this as medicine, not as a supplement.
- 📍 Visit us at Perfect B | 3905 NW 107th Ave, Suite 104, Doral FL 33178
- 📞 Call or message us at (786) 502-2260
- 💳 Buy Now Pay Later available: Cherry, Klarna, Afterpay, CareCredit
→ Book your peptide consultation for women over 40 at Perfect B in Doral today.


