
Perfect B, Doral Fl. | 06.30.26 | 11 min read.
This article is for general education and is not medical advice; please consult your OB and a qualified provider before starting or stopping any treatment, especially while pregnant or breastfeeding.
You made it through pregnancy, and then a few weeks after delivery your skin turned on you: deep, tender bumps along the jaw and chin, breakouts in places you have not seen since your teens. If this is you, take a breath. Postpartum acne is real, extremely common, and not a sign that you did anything wrong. It is your hormones rearranging themselves, and there is a clear, safe path forward whether you are nursing now or already weaning. At Perfect B in Doral, we walk new mothers through this every week, and this guide gives you the same plan we share in person.
Key Takeaways
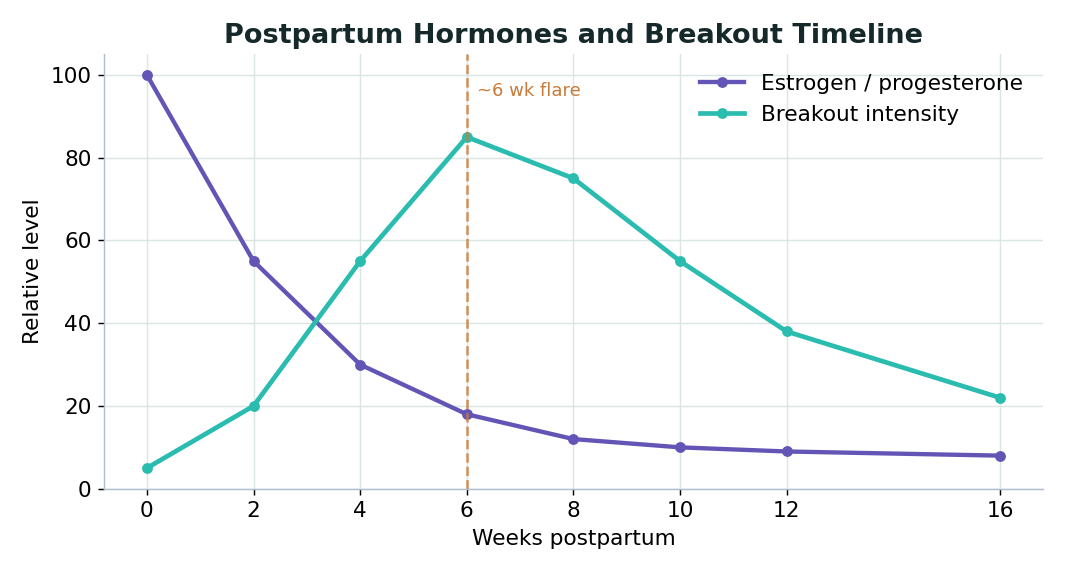
- Postpartum acne is usually driven by the rapid drop in estrogen and progesterone after birth while androgens stay relatively higher, often showing up around six weeks postpartum as cysts along the jawline and chin.
- This is hormonal, not hygiene. It is not your fault, and gentle, consistent care beats aggressive scrubbing.
- While breastfeeding, care stays in a safe lane: azelaic acid, niacinamide, a gentle cleanser, mineral SPF, limited topical benzoyl peroxide discussed with your provider, and gentle in-clinic facials.
- After you have fully weaned, the stronger toolkit opens up: prescription tretinoin, a salicylic acid peel series, and spironolactone for stubborn hormonal jawline cysts, all after a provider evaluation.
- South Florida sun plus postpartum hormone shifts can also trigger melasma, so daily non-comedogenic mineral SPF is part of the plan from day one.

What exactly is postpartum acne and why does it happen?
Postpartum acne is acne that appears or worsens in the weeks and months after you give birth. Picture the hormonal roller coaster of pregnancy and then the sudden stop. Estrogen and progesterone climb to very high levels during pregnancy, then fall fast after delivery. Androgens, the hormones tied to oil production, do not drop the same way, so for a window of time your skin runs with relatively higher androgen influence and far less of the estrogen that had kept things calm.
That shift is the engine behind postpartum breakouts: higher relative androgen activity tells your oil glands to produce more sebum, and extra oil combined with pore-lining cells and skin bacteria sets the stage for clogged pores and inflamed cysts. This is why so many women notice the change around six weeks postpartum, and why the breakouts cluster along the lower face, jaw, and chin, the classic map of hormonal acne after pregnancy. If you sailed through pregnancy with clear skin and then suddenly flared, you are not imagining it.
“The hormonal crash after birth can trigger a whole new wave of breakouts. Some women who sailed through pregnancy with glowing skin suddenly flare around six weeks postpartum. The message I want every new mom to hear is that this is not her fault, it is hormones rearranging everything, there is no guilt and no judgment, and we have a bridge plan that keeps both her skin and her baby safe.”
Valeria Marulanda, FNP-BC, Perfect B Aesthetics, Doral
Is this the same acne I had during pregnancy?
Not always, and the difference matters. Some women break out during pregnancy itself, usually in the first trimester. If that was your story, read our companion guide on what to do about acne during pregnancy and which treatments are considered safe before you deliver, because the safe list overlaps but the timing differs. Pregnancy acne is the climb; postpartum acne is the drop. Other women stay clear the whole pregnancy and only break out afterward, the hormonal crash pattern we focus on here.
When does postpartum acne usually start, and how long does it last?
No single calendar fits everyone, because your hormones, genetics, and how long you breastfeed all shape the timeline, but there is a typical arc. In the first few weeks, hormones are just beginning to fall and skin often still looks fine. Around six weeks postpartum is the common flare point, when jawline and chin cysts appear as estrogen drops. Through months two to six the breakouts may persist or fluctuate, sometimes worsened by sleep loss and stress. As you approach and finish weaning, hormones normalize and the stronger toolkit becomes appropriate after a provider evaluation. Breastfeeding can extend this window, so do not be discouraged if yours runs longer.
For many women the breakouts calm down within several months as hormones rebalance; for others, especially those prone to hormonal acne, it digs in and needs treatment. Neither outcome reflects how well you care for your skin. It reflects your hormone biology, which is largely out of your hands.
What is safe to use on postpartum acne while you are still breastfeeding?
This is the question we hear most, and it deserves an honest answer, because what reaches your bloodstream can in small amounts reach your milk. The principle is simple: while you are nursing, we keep treatment in a safe lane and coordinate with your OB, treating the skin you have now with gentle ingredients and saving the stronger plan for after you wean. Here are the breastfeeding-safe building blocks we lean on; always confirm your situation with your OB and provider first.
- Azelaic acid: a workhorse for acne while breastfeeding that calms inflammation, clears clogged pores, and can fade the dark marks that linger on deeper skin tones. Generally considered compatible with nursing, but discuss it with your provider first.
- Niacinamide: a gentle, barrier-supporting ingredient that helps regulate oil and reduce redness without irritation. We explain why we love it in our guide to the skin barrier benefits of niacinamide for acne-prone and sensitive skin.
- A gentle, non-stripping cleanser, twice daily, no scrubbing. Harsh cleansers damage your barrier and make postpartum breakouts worse.
- Mineral SPF with zinc oxide or titanium dioxide: non-negotiable and non-comedogenic, for the Florida reason below.
- Topical benzoyl peroxide, in limited spot use: because it is applied sparingly, it is sometimes considered an option while nursing, but discuss it with your provider first and keep it off any area your baby’s skin contacts.
- Gentle in-clinic facials and HydraFacial style treatments: a safe way to deep clean congested skin and calm inflammation while you are nursing.

What should I avoid or postpone while breastfeeding?
These are the treatments we typically hold until after you have fully weaned, or use only with explicit OB and provider clearance. Being conservative protects both you and your baby.
- Oral spironolactone: excellent for hormonal jawline cysts, but generally postponed while breastfeeding. We plan for it, we do not start it yet.
- Oral isotretinoin: not appropriate while breastfeeding. It requires you to be done nursing and under close supervision.
- Topical retinoids such as tretinoin: generally avoided while nursing as a precaution, one of the biggest differences between the two plans.
- Strong salicylic acid chemical peels: usually deferred; gentle in-clinic facials are a safer alternative in the meantime.
The point is not to leave you with no options. It is that you have a real, breastfeeding-safe routine now, and a clearly mapped stronger plan waiting the moment you are ready.
While breastfeeding versus after weaning: what is actually safe?
Because this distinction is so important and so easy to get confused about online, here is a side by side comparison you can screenshot and bring to your appointment. Treat it as a conversation starter with your provider, not a substitute for personalized clearance.
| Treatment | While breastfeeding | After fully weaning |
|---|---|---|
| Azelaic acid | Generally considered compatible; discuss with your provider | Continue as needed |
| Niacinamide | Gentle and well tolerated | Continue as needed |
| Gentle cleanser and mineral SPF | Yes, foundational | Yes, foundational |
| Topical benzoyl peroxide | Limited spot use; discuss with your provider | Available as needed |
| Gentle in-clinic facials and HydraFacial | Yes, a safe favorite | Yes |
| Topical tretinoin and other retinoids | Generally avoided; only with provider and OB clearance | Appropriate after provider evaluation |
| Salicylic acid peel series | Usually deferred | Appropriate after provider evaluation |
| Oral spironolactone | Generally postponed; discuss with your provider and OB | An option for hormonal jawline cysts after evaluation |
| Oral isotretinoin | Not appropriate while breastfeeding | Considered only after weaning, under close supervision |
One honest caveat: research on what crosses into breast milk and at what dose is limited for many of these products, which is exactly why the safe answer is to coordinate with your OB and provider rather than assume. To read the science yourself, the literature indexed on PubMed, the National Library of Medicine database of peer-reviewed research, is a good start, and the patient education from the American Academy of Dermatology on acne causes and treatments is reliable and current.
What is the “go full force” plan after you have weaned?
This is the part that gives so many of our patients hope. The breastfeeding season does not last forever, and when it ends, the full toolkit opens up. We make a tentative plan early and write it in the chart so you can reach out when ready.
“I always have the postpartum chat: once you deliver and you are done breastfeeding, come back and we go full force. We make a tentative plan, maybe a salicylic acid peel series, maybe prescription tretinoin, maybe spironolactone if the jawline cysts return, and I write it in the chart so the patient reaches out when she is ready. While she is still nursing we keep it safe: azelaic acid, niacinamide, a gentle cleanser, mineral SPF because melasma loves the hormone shifts, and gentle in-clinic facials.”
Valeria Marulanda, FNP-BC, Perfect B Aesthetics, Doral
Once a provider evaluation confirms you are fully weaned and a good candidate, the stronger options typically include:
- Prescription tretinoin: a topical retinoid that speeds cell turnover, unclogs pores, and improves texture and post-acne marks over time. One of the most effective tools we have, appropriate once you are no longer nursing.
- A salicylic acid peel series: a course of in-clinic peels that deep clean pores, calm active breakouts, and smooth the skin. A series spaced over weeks tends to outperform a single treatment.
- Spironolactone for hormonal jawline cysts: an oral medication that addresses the androgen-driven oil behind those stubborn lower-face cysts. If your jawline acne returns after weaning, this is often the missing piece, and a cornerstone of how we approach preventing recurring hormonal breakouts along the jaw and chin.
We tailor the order and combination to your skin, your history, and your goals. Some women need only one of these; others do best with a thoughtful combination. The plan is yours, and it waits for you.
Why does South Florida sun make postpartum skin care different?
Here in Doral and across South Florida, the sun is intense nearly year round, and that changes the postpartum skin equation in two ways. First, the same hormone swings that drive postpartum breakouts also make skin more prone to melasma, the patchy brown discoloration that loves estrogen shifts and the postpartum period; strong Miami sun is melasma’s best friend, and once it sets in, it is stubborn. Second, several acne treatments make skin more sun sensitive.
The fix is the same for both, and you can start it today, even while breastfeeding: a daily non-comedogenic mineral sunscreen with zinc oxide or titanium dioxide, worn every morning, rain or shine. Mineral formulas sit on top of the skin and are generally the gentle, nursing friendly choice. For a new mom in South Florida, sunscreen is not a luxury step. It is part of the treatment.
What can you do at home to help postpartum breakouts right now?
You are exhausted, touched out, and short on time, and the good news is you do not need a ten step routine. A short, consistent, gentle routine beats an elaborate one you cannot keep up with. Here is a realistic framework.
- Cleanse gently twice a day with a mild cleanser, lukewarm water, and your fingertips. Skip scrubs and harsh foaming washes that strip your barrier.
- Apply your safe actives. Azelaic acid and niacinamide are your friends; introduce one at a time so you can tell what works.
- Moisturize. Oily, acne-prone skin still needs hydration; a lightweight, non-comedogenic moisturizer keeps your barrier intact.
- Sunscreen every morning. Mineral and non-comedogenic, the Florida step you cannot skip.
- Do not pick. Squeezing cysts spreads inflammation and risks scars and dark marks that take far longer to fade than the breakout itself.
- Wash what touches your face: pillowcases, phone screens, and the muslin cloths that end up everywhere with a newborn.
And give yourself grace. Sleep, hydration, and a few minutes of calm support both your skin and you.
When should you see a provider about postpartum acne?
Mild congestion that responds to gentle care can often be managed at home, but some signs mean it is worth getting professional eyes on your skin sooner: deep or painful cysts and nodules, acne that is leaving scars or dark marks, breakouts not improving after several weeks of gentle care, or skin changes affecting your confidence and mood during an already vulnerable time. There is no prize for waiting it out alone. A provider can confirm what is driving your breakouts, build a breastfeeding-safe plan now, and map the after-weaning plan for when you are ready.

Frequently asked questions about postpartum acne
1. When does postpartum acne usually start?
It commonly appears around six weeks after birth, when the drop in estrogen and progesterone is well underway while androgens remain relatively higher. Some women notice it earlier or later, and breastfeeding can extend the window. The jaw and chin are the most common spots.
2. Is acne while breastfeeding normal, and is it safe to treat?
Yes to both, as long as you stay in the safe lane and coordinate with your OB and provider. Breastfeeding-safe postpartum acne treatment usually means azelaic acid, niacinamide, a gentle cleanser, mineral SPF, limited topical benzoyl peroxide, and gentle in-clinic facials. The stronger oral and retinoid options wait until weaning.
3. Can I use retinol or tretinoin for hormonal acne after pregnancy while nursing?
Topical retinoids such as tretinoin are generally avoided while breastfeeding as a precaution, one of the biggest differences between the two plans. Once you have weaned and a provider confirms you are a candidate, prescription tretinoin becomes one of the most effective tools we have.
4. Will my postpartum breakouts go away on their own?
For many women they calm down within several months as hormones rebalance, often around weaning. For others, especially those prone to hormonal acne, they persist and need treatment. If it is painful or not improving, see a provider.
5. What is the best postpartum acne treatment once I have finished breastfeeding?
After weaning and a provider evaluation, the stronger toolkit typically includes prescription tretinoin, a salicylic acid peel series, and spironolactone for hormonal jawline cysts, combined to fit your skin and goals.
6. Why do I have acne now when my skin was perfect during pregnancy?
Because pregnancy and postpartum are opposite hormone movements. High estrogen often keeps skin calm during pregnancy; after birth it falls fast while androgens stay relatively higher, ramping up oil and triggering breakouts. Clear pregnancy skin followed by a flare is classic.
7. Do these breakouts mean my hormones are unbalanced or that something is wrong?
Not necessarily. The postpartum hormone shift is a normal, expected process, and the acne it causes is a normal response, not a sign you did something wrong. If breakouts are severe or paired with other symptoms, a provider can evaluate whether anything else is contributing.
Closing: Two Plans, One Bridge
Postpartum acne is not your fault, and you do not have to white-knuckle through it. Whether you are six weeks out and nursing, or just weaned and ready to go full force, there is a safe and effective plan for the stage you are in right now, plus a clear map for the next one.
The bridge from breastfeeding-safe care to the full-force plan is a conversation we have at your first visit at Perfect B in Doral, so you are never starting from scratch when the hormones shift again. Both phases go into your chart from day one.
- 📍 Visit us at Perfect B, 3905 NW 107th Ave, Suite 104, Doral FL 33178
- 📞 Call or message us at (786) 502-2260
- 💳 Financing available through Cherry, Klarna, Afterpay, and CareCredit


