

Perfect B, Doral Fl. | 05.06.25 | 8 min read.
This post is for educational purposes only and does not constitute medical advice. Cystic acne is a clinical condition that requires evaluation by a licensed provider. The information below reflects clinical experience at Perfect B and published medical literature. Always consult a qualified provider before starting any treatment.
What Makes Cystic Acne Different From Every Other Breakout?
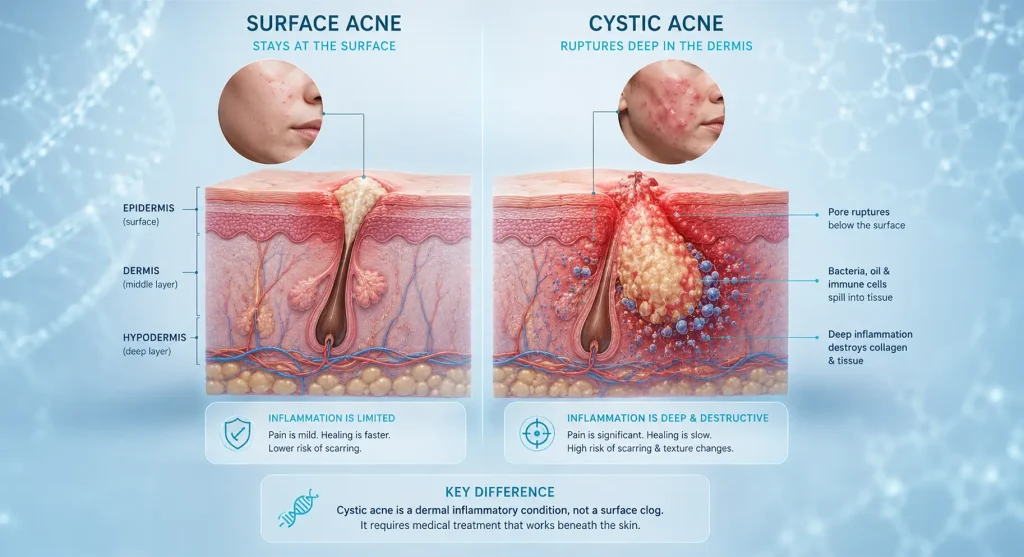
Most acne starts at the skin’s surface. Cystic acne starts below it. When a pore ruptures deep in the dermis, bacteria, oil, and dead skin cells spill into surrounding tissue. Your immune system registers this as an injury and sends a flood of inflammatory cells to contain it. That inflammatory response presses directly on nerve endings, which is why a cystic nodule throbs and aches in a way a regular whitehead never does.
→ Gut health is one of the most overlooked internal drivers of persistent inflammatory acne, for a complete breakdown of how gut dysbiosis contributes to breakouts and what the gut-skin axis means for treatment, read our guide to gut health and acne at Perfect B in Doral.
This is also why cystic acne and treatment need to be discussed together from day one, not after months of topicals that produce no result. Every active cyst is destroying collagen in the surrounding tissue while the inflammation works through the repair cycle. By the time the cyst resolves, it leaves either a textural depression, a dark spot, or both. That damage is permanent without clinical intervention.
Understanding this changes the conversation entirely. You are not dealing with a clogged pore that a better cleanser or stronger benzoyl peroxide will fix. You are dealing with a wound below the surface that requires clinical-level targeting to stop and reverse. In South Florida, we regularly see patients in their mid-20s who spent three or four years managing cystic acne with over-the-counter products, arriving at the clinic with significant scarring that early intervention would have prevented.
Key Takeaways
- Cystic acne is a dermal wound, not a surface problem. The pore ruptures below the skin, which is why topical products cannot reach the source of the inflammation.
- The best acne treatment for cystic acne starts with bloodwork, not a prescription. Hormonal labs before any oral medication changes the precision of everything that follows.
- Every untreated cyst destroys collagen. Early clinical care is the only way to prevent permanent scarring. Waiting months is the most common reason we see deep textural damage in patients under 30.
- Spironolactone is the most effective non-antibiotic option for women with hormonal cystic acne. It blocks androgen receptors at the sebaceous gland level without the long-term resistance risk of antibiotics.
- Scar repair is a separate phase. Microneedling for acne scars and cystic acne laser treatment begin only after active breakouts are fully controlled, typically 3 to 6 months into the protocol.
Why Your Cleanser and Benzoyl Peroxide Cannot Reach the Problem
Benzoyl peroxide penetrates the pore and kills bacteria. Salicylic acid exfoliates dead skin cells to prevent congestion. Both of these mechanisms operate at the skin surface or just beneath it. Cystic acne causes ruptures in the dermis, which sits significantly deeper than where any topical ingredient acts.
This is the single most important concept for anyone frustrated by years of skincare products with no improvement. The failure was not about product quality or inconsistent application. The failure was anatomical. The target was simply unreachable from the surface.
Once patients understand this, two things happen: they stop blaming their skincare routine, and they stop delaying clinical care. That delay is where the permanent damage accumulates. A patient who waits six months before seeking evaluation for cystic acne treatment is a patient who arrives with scarring that now requires its own separate treatment phase.
The Hormone Connection: Why Most Cystic Acne Is a Hormonal Acne Treatment Case
Androgens, specifically testosterone and DHEA-S, stimulate sebaceous glands to produce excess sebum. When sebum production outpaces what the pore can drain, pressure builds and the pore wall ruptures. Elevated insulin compounds this by amplifying androgen activity, which is why high-sugar and high-dairy dietary patterns often correlate with flare cycles.

The location of breakouts is a direct clinical signal. Cystic acne on the jawline, concentrated along the jaw and chin and following a monthly hormonal cycle, is almost always driven by androgen excess. At Perfect B, hormonal acne treatment begins with bloodwork, not a prescription pad. We check testosterone, DHEA-S, fasting insulin, and vitamin D before recommending any oral medication. Nine times out of ten, the labs reveal at least one marker that is elevated or suboptimal. That information changes the protocol completely.
Patients who have been told their hormones are “normal” by a general practitioner often arrive with no further direction. What “normal” means in a standard reference range is not the same as optimized for sebaceous gland function. Functional evaluation looks at ratios and ranges specific to hormonal acne presentations, not population averages. A 2017 review published in the International Journal of Women’s Dermatology confirming that androgen excess is a primary driver of hormonal acne in adult women and that anti-androgen therapy significantly reduces cyst formation supports labs-first evaluation as the clinical standard for this presentation.
How We Approach Cystic Acne Treatment at Perfect B in Doral, FL
The best acne treatment for cystic acne is not a single intervention. It is a protocol that addresses the inflammatory response, the hormonal trigger, and the surface congestion simultaneously, in a specific order. Here is how Victoria structures that at Perfect B.
Step 1: Calm the Inflammation Fast
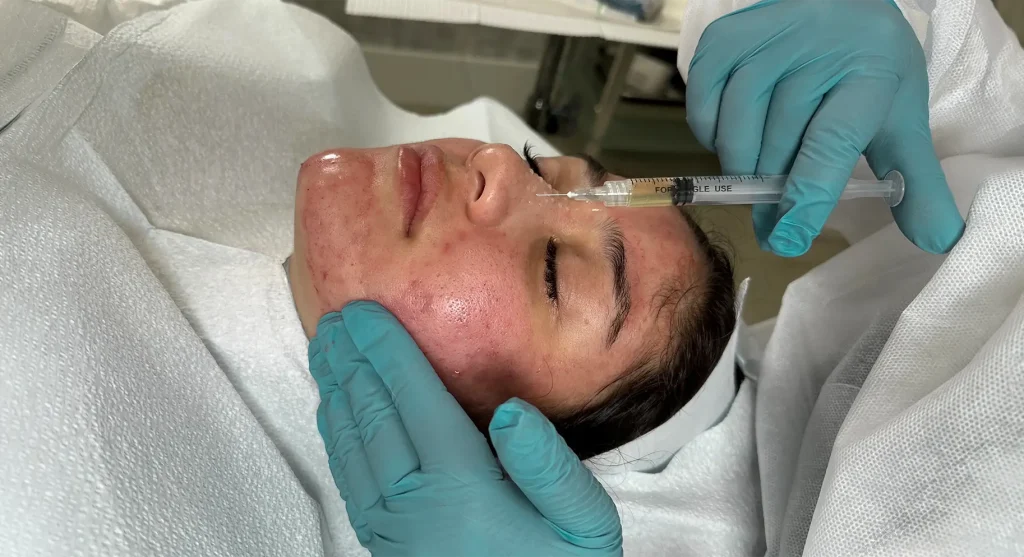
When a patient arrives with a painful active cyst, the first priority is reducing inflammation as quickly as possible. A cortisone injection for acne delivers triamcinolone directly into the nodule, shrinking the cyst within 24 to 48 hours and significantly reducing the risk of scarring at that site by interrupting the inflammatory cascade before it fully damages the surrounding collagen. This is not a long-term solution, but it is the right move for an emergency presentation or a cyst that has been building for weeks with no resolution.
In Victoria’s words: “When a patient sits in my chair with a painful cyst, the first thing I do is calm the inflammation fast, usually with a cortisone injection. You cannot build a long-term protocol on top of active fire.”
Step 2: Run Labs Before Prescribing Anything
Before any oral medication, the clinic pulls testosterone, DHEA-S, fasting insulin, and vitamin D. We are looking for androgen excess, insulin resistance, and nutrient deficiencies that are compounding the inflammatory load. This step takes one additional visit but changes the precision of everything that follows. A patient with high DHEA-S and normal testosterone gets a different protocol than one with elevated insulin and low vitamin D. Treating all cystic acne identically is precisely why so many patients cycle through protocols that never fully work.
Step 3: Spironolactone, Tretinoin, and the Clinical Core
For women with confirmed androgen excess, spironolactone for acne is the most effective non-antibiotic option available. It blocks androgen receptors in the sebaceous glands, reducing sebum output at the hormonal source rather than treating downstream effects. The typical result is a significant reduction in new cyst formation within 8 to 12 weeks. Paired with topical tretinoin, which accelerates cell turnover, keeps pores clear, and begins stimulating collagen in damaged areas, this combination addresses both the hormonal driver and the surface congestion simultaneously.
On isotretinoin, Victoria is direct: “I don’t jump straight to isotretinoin unless nothing else is moving the needle after a solid 3 to 4 months, or the scarring is aggressive and we cannot afford to wait. Some cases need the big gun, and I will refer out when that is the right call.”
What Realistic Results Look Like in the First 60 to 90 Days
Cystic acne did not develop overnight, and the hormonal and inflammatory cycles driving it take time to recalibrate. Here is what a well-managed protocol produces in the first three months.
- Weeks 1 to 4: Cortisone injections address existing active cysts. Spironolactone begins blocking androgen activity. Tretinoin starts accelerating cell turnover. The skin may purge slightly as surface congestion resolves.
- Weeks 4 to 8: New cyst formation slows significantly. Frequency and severity of breakouts decreases. Existing inflammation fades. Patients consistently describe the skin as “quieter,” which is accurate at this stage.
- Weeks 8 to 12: Active breakouts are substantially reduced. Redness has faded. The skin is stable enough to evaluate what remains in terms of scarring and pigmentation, and what the repair phase requires.
The skin will not be flawless at 90 days. What it will be is calm, which is the precondition for everything that follows. Attempting scar treatment on actively inflamed skin is counterproductive, which is why this stabilization phase is non-negotiable.

When Isotretinoin Is the Right Call
Isotretinoin remains the most effective oral treatment for severe scarring cystic acne. It reduces sebaceous gland output dramatically and can produce long-term remission in cases that have not responded to other interventions. At Perfect B, it is not a first-line treatment.
The criteria for isotretinoin referral include: active cysts continuing to form after 3 to 4 full months on spironolactone and tretinoin, aggressive scarring progressing faster than conservative treatment can manage, or a clinical picture where continuing to wait creates irreversible collagen damage. When it is the right call, the referral is made directly rather than extending protocols that are insufficient for the severity of the case.
Getting Rid of the Scarring Once Active Cysts Are Under Control
Cystic acne scarring is a separate clinical problem from active acne. It requires a separate treatment phase that does not begin until active breakouts are controlled. Attempting scar repair while cysts are still forming wastes clinical resources and introduces inflammatory conditions that slow the repair response. Once the skin is stable, typically 3 to 6 months into a managed protocol, the scar pattern is evaluated and the appropriate intervention recommended.
Microneedling for Acne Scars
SkinPen microneedling for acne scars creates controlled micro-injuries in the dermis that trigger the skin’s natural collagen production response. Each session deposits new collagen in the exact areas where cystic inflammation previously destroyed it. For rolling scars and shallow boxcar scars, three to four sessions spaced four to six weeks apart typically produce visible improvement. Results continue developing for three to six months after the final session as collagen remodeling completes. A 2015 clinical study published in the Journal of Cutaneous and Aesthetic Surgery demonstrating that microneedling produces statistically significant improvement in acne scar depth and texture with a favorable safety profile across all Fitzpatrick skin types supports this as a first-line option for most patients.
Cystic Acne Laser Treatment
Cystic acne laser treatment is appropriate for deeper scar patterns that do not respond adequately to microneedling alone. Fractional laser creates columns of controlled thermal injury in the dermal layer, stimulating aggressive collagen remodeling. For ice pick and deep boxcar scars, laser produces more significant structural change than needling, though with a longer recovery period. Skin tone and Fitzpatrick classification are evaluated before recommending laser, since certain wavelengths carry pigmentation risks in darker skin tones that require specific protocols.
Chemical Peels for Texture and Pigmentation
Chemical peels address the repair phase only, never the active phase. TCA and salicylic-based peels at clinical concentrations accelerate turnover of pigmented surface cells and improve skin uniformity. Most patients in the repair phase benefit from two to four peel sessions spaced three to four weeks apart, used alongside microneedling or laser as part of a combined approach. As Victoria states directly: “Don’t peel over an angry, inflamed bump. You will make it worse. Peels are for the aftermath.”

Lifestyle Triggers That Make Cystic Acne and Treatment Harder in Miami
Lifestyle does not cause cystic acne. But it amplifies the hormonal and inflammatory drivers that produce it. In South Florida, the patterns seen most consistently in patients with hard-to-control breakouts include high dairy intake, excess refined sugar, chronic stress, and disrupted sleep.
Dairy, particularly cow’s milk and whey protein, raises IGF-1, which stimulates androgen production and increases sebum output. Patients who swap cow’s milk for oat milk and eliminate whey protein from their supplement routine frequently report a measurable reduction in breakout frequency within four to six weeks, even before clinical treatment takes full effect. It is not a replacement for treatment. It reduces the baseline inflammatory load the protocol has to work against.
The Miami lifestyle adds specific variables: late nights, elevated cortisol from chronic stress, alcohol, and the hormonal disruption that follows poor sleep. Cortisol directly stimulates androgen production. A patient sleeping five hours a night and drinking three nights a week is working against their clinical protocol every single day. Victoria is specific: track food intake for 48 hours before a flare, eliminate dairy and refined sugar, protect sleep, and cut whey. Small targeted changes move the needle when combined with a real clinical plan, not in isolation.
Frequently Asked Questions
1. What is cystic acne and why does it hurt so much?
Cystic acne is the deepest type of breakout. The pore ruptures below the surface of the skin, deep in the dermis rather than at the surface. That deep inflammation presses directly on nerve endings, which is why it throbs and causes real pain in a way surface breakouts never do. It is anatomically a tiny internal wound, and the body responds to it exactly as it responds to any tissue injury.
2. Can cystic acne be treated without antibiotics?
Yes. At Perfect B, spironolactone, custom topicals, cortisone injections for acute management, and in-office procedures produce consistent results without long-term antibiotic use. Antibiotics have a role in certain acute presentations, but they are not the foundation of how cystic acne treatment is approached today, and their long-term use carries resistance risks that matter.
3. Does a chemical peel help with cystic acne?
Not for active cysts. Applying a peel to inflamed, active skin worsens the inflammation and increases the risk of post-inflammatory hyperpigmentation. Peels are a repair-phase tool. They address scarring, pigmentation, and texture that remain after cysts have resolved. The sequencing matters: peels belong in phase two, not phase one.
4. How many sessions are needed to see improvement?
For active cysts, a well-managed protocol produces visible improvement within four to eight weeks. For scarring, three to six sessions of microneedling or laser spaced four to six weeks apart, depending on scar depth and type. Collagen remodeling continues for months after the final session.
5. Does cystic acne always leave scars?
Pretty much, especially if you mess with it. The inflammation destroys collagen and leaves either a dent or a dark spot. Early treatment is the only way to minimize it. Popping one yourself is a guaranteed scar.
6. Is cystic acne hormonal?
Most of the time, yes. Especially if it is clustered on the jaw and chin and cycles with your period. We always run hormone labs on cystic patients. The answer is usually sitting in their bloodwork.
7. Can diet cause cystic acne?
It can trigger it. Big culprits: dairy, sugar, and for some people, whey protein or peanut butter. It is not the root cause but it definitely pours gas on the fire. Track what you ate 48 hours before a flare and the pattern usually shows up fast.
8. What cystic acne treatment does Perfect B offer in Miami?
We do it all: lab work to find the trigger, prescription topicals and orals like spironolactone, cortisone shots for quick relief, and then cystic acne laser treatment, peels, and microneedling for acne scars once the skin is stable. Full spectrum. We treat the inside and the outside. Call our Doral, FL clinic at (786) 502-2260 to schedule an evaluation.
The Clinical Bottom Line on Cystic Acne
Cystic acne is one of the most damaging conditions treated at Perfect B, not because it is medically dangerous, but because the window for preventing permanent scarring is narrow and easy to miss. Every week spent managing deep breakouts with over-the-counter products is a week of collagen loss that cannot be recovered without clinical scar treatment later.
The patients who arrive with the best outcomes are the ones who came in early, ran the labs, started the best acne treatment for cystic acne that matched their hormonal profile, and gave it the full 60 to 90 days to stabilize before evaluating what the repair phase requires. If you have been through the cleanser rotation, tried multiple topical regimens, and still have active cystic breakouts, the issue is not your skincare. The target is below the surface and requires a clinical approach.
📍 Visit us at Perfect B, Doral FL, for a clinical evaluation built around your labs, not a generic skin type.
📞 Call or message us at (786) 502-2260


