

Perfect B, Doral Fl. | 06.16.26 | 10 min read.
This post is for educational purposes only and does not substitute for personalized medical advice. Acne treatment in Fitzpatrick III to VI skin requires customization to avoid post-inflammatory hyperpigmentation. Speak with our team before starting any active protocol.
Key Takeaways
- Acne on dark skin is a pigmentary problem first: the breakout heals in weeks, the dark mark that follows lasts months. The protocol must protect against post-inflammatory hyperpigmentation as much as it clears the acne.
- Aggressive standard protocols often backfire: high-strength benzoyl peroxide, harsh exfoliants, and aggressive retinoids can clear surface lesions while triggering long-term PIH in Fitzpatrick III to VI skin.
- Barrier-first beats actives-first: for skin of color, repairing the barrier and calming inflammation before adding active ingredients delivers faster cosmetic clearance.
- Azelaic acid plus salicylic acid plus niacinamide is the working baseline: these three address acne, inflammation, and pigment in parallel without the PIH risk of more aggressive options.
- In-clinic procedures must be Fitzpatrick-matched: chemical peels, RF microneedling, and certain lasers can help, but device selection and settings change for darker skin.
Why Dark Skin Acne Treatment Is Fundamentally Different
Acne in black skin and acne in lighter skin look similar in the mirror. The cellular response is not the same. Three biological differences shape every clinical decision when treating acne in skin of color at our Doral, FL clinic.
- Melanocyte responsiveness: Fitzpatrick III to VI skin contains more melanocytes that release more pigment in response to any inflammatory trigger. The acne lesion can resolve completely and leave a dark mark that persists for 6 to 18 months.
- Inflammatory threshold: the same dose of an active ingredient that produces mild irritation in Fitzpatrick II skin can produce significant pigmentary inflammation in Fitzpatrick V. The protocol must respect this differential sensitivity.
- Barrier function: darker skin has measurable differences in transepidermal water loss patterns, ceramide composition, and pH response. Generic acne routines optimized for Fitzpatrick II skin can leave skin of color barrier-compromised.
A 2022 peer-reviewed review in PubMed Central on managing acne in skin of colour, including the unique inflammatory and pigmentary considerations that change first-line treatment selection for Fitzpatrick IV to VI patients confirms that the pigmentary sequelae of acne, not the acne itself, drive most long-term clinical concerns for these patients.
The 4 Mistakes That Make Acne in Black Skin Worse
- Brute-force benzoyl peroxide for everything: benzoyl peroxide on dark skin can dry the surface enough to inflame the dermis, leaving a brown footprint where each lesion sat. Use it as a targeted spot treatment, not as an all-over wash.
- Skipping moisturizer to dry out breakouts: dry, compromised skin pigments faster. Skipping the moisturizer step accelerates PIH and slows the actual clearance.
- Starting retinoids at full strength: tretinoin or retinol at standard concentrations can trigger a purge phase that pigments aggressively in skin of color. Start low, build slow, never skip barrier support.
- No daily sunscreen: the dark marks deepen every day they see UV. South Florida sun is unforgiving on inflamed skin. Mineral SPF 30 or higher is part of the treatment, not optional.
Harvard Health’s clinical guidance on acne considerations for darker skin tones, detailing why aggressive standard acne protocols frequently trigger post-inflammatory hyperpigmentation in Fitzpatrick III to VI patients and how to sequence treatment to prevent it aligns directly with the barrier-first protocol our Doral clinic uses on Hispanic and Latin patients every week.
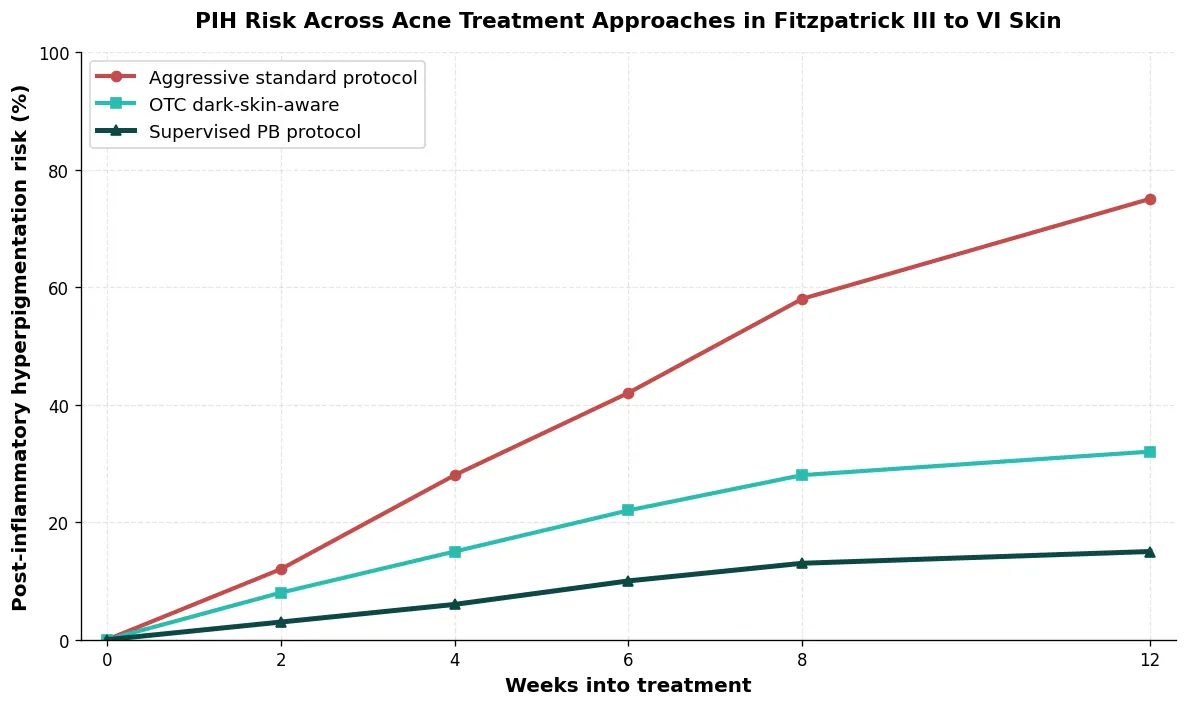
Side-by-Side: PIH Risk Across Acne Approaches
The chart below maps observed post-inflammatory hyperpigmentation risk across three treatment paths over 12 weeks in Fitzpatrick III to VI patients at our Doral clinic. Aggressive standard protocols clear lesions but at a steep pigment cost. Dark-skin-aware OTC reduces the trade-off. A supervised clinical protocol keeps PIH risk minimal while still clearing acne.
The Layered Protocol Perfect B Uses for Fitzpatrick III to VI
Our Doral clinic builds dark skin acne treatment protocols around four anchor ingredients and a barrier-first sequence. These are the layers, in the order we introduce them.
- Gentle cleanser with 2 percent salicylic acid: salicylic acid for dark skin is well tolerated and reaches into the pore without sandpapering the surface. Our complete clinical guide to using salicylic acid for acne, including daily-use protocol, concentration ladder, and when BHA outperforms benzoyl peroxide in skin of color details the exact dosing logic.
- Azelaic acid 10 to 15 percent: azelaic acid on dark skin is a dual-action ingredient that addresses both acne and pigment at once. It inhibits tyrosinase activity, which means it can prevent and fade dark marks while clearing acne, without the irritation risk of hydroquinone.
- Niacinamide serum 5 to 10 percent: reduces inflammation, normalizes sebum, and supports the barrier. Our breakdown of how niacinamide actually works at the cellular level for acne-prone, redness-prone, and barrier-compromised skin covers the dose-response and stacking notes that matter for Fitzpatrick III to VI.
- Ceramide and hyaluronic acid moisturizer: fragrance-free, non-comedogenic, twice daily. Barrier integrity is the firewall against PIH.
- Mineral SPF 30 or higher daily: zinc oxide or titanium dioxide based. Chemical filters can sting compromised skin. Tinted mineral options blend better on Fitzpatrick IV and above.
- Retinoid only after barrier is stable: introduce low-strength adapalene or retinol 0.3 percent only after the skin tolerates the baseline protocol for 4 to 6 weeks.

In-Clinic Procedures Safe for Dark Skin Acne in Miami
Procedural acne treatments can accelerate clearance and address scarring, but device selection and settings matter enormously in Fitzpatrick III to VI. What works on light skin can pigment darker skin. These are the procedures our Doral clinic uses for skin of color acne, and the ones we approach carefully.
- Chemical peels: yes, with care. Salicylic acid peels and azelaic acid peels at low concentrations work well in Fitzpatrick III to V. Glycolic peels require dose adjustment. We start gentle and build tolerance.
- RF microneedling: yes. Radiofrequency microneedling for dark skin acne and acne scarring delivers thermal energy without surface chromophore targeting, which makes it one of the safer procedural options for Fitzpatrick IV to VI.
- Q-switched and picosecond lasers: case-by-case. For acne scarring and PIH, these can help with the right wavelength selection. Aggressive ablative lasers are rarely first-line in darker skin.
- HydraFacial and gentle extractions: yes. Vortex extraction clears comedonal acne without the friction of manual extractions that can trigger inflammation.
- Aggressive ablative resurfacing: rarely. Full CO2 ablation in Fitzpatrick V to VI carries a high PIH risk. We reserve it for specific cases with informed consent and a slow ramp.
Treating Existing Dark Spots Without Triggering New Ones
Most patients who walk into our Doral clinic for dark skin acne treatment in Miami arrive with two problems at once: active acne and a constellation of post-inflammatory dark marks from previous breakouts. Treating both at the same time is possible if the protocol respects the inflammation budget.
- Pigment-targeted ingredients that double as acne actives: azelaic acid, niacinamide, and tranexamic acid topical formulations fade dark marks while supporting acne management.
- Stronger pigment correctors come after the barrier holds: kojic acid, alpha arbutin, and prescription-strength options enter the routine after the baseline protocol has stabilized.
- For deeper PIH and acne scarring: see our complete clinical guide to post-inflammatory hyperpigmentation in skin of color, including ingredient ladders, in-office procedures, and realistic fade timelines for Fitzpatrick III to VI patients.
- Patience is part of the protocol: PIH fading takes 3 to 12 months even with the right tools. Aggressive shortcuts create new dark marks faster than they fade old ones.
Daily Routine for South Florida Hispanic and Latin Patients
The acne hispanic skin and acne latina skin patient base in Miami brings a specific cluster of considerations: high humidity, intense year-round sun, mixed Fitzpatrick III to V skin, and lifestyle patterns that include extended outdoor time. The routine below is what we build for most patients at our Doral clinic, adjusted per individual.
- Morning: Gentle cleanser, niacinamide serum, ceramide moisturizer, mineral SPF 30 or higher.
- Evening: Salicylic acid cleanser, azelaic acid layer, moisturizer. Skip actives if skin is irritated, hold the line until barrier recovers.
- Weekly (week 6 onward): Add a gentle exfoliating treatment such as a PHA cleanser once per week. Avoid scrubs.
- Post-sun-exposure: Cool shower, gentle cleanser, soothing niacinamide, reapply SPF if going back out.
- Acne flare days: Spot-treat with benzoyl peroxide, keep the rest of the routine identical. Do not escalate the whole face for one or two lesions.
For patients who want the full clinic-supervised path with in-office procedures stacked on the home routine, see our complete Acne Treatment Plan at Perfect B in Doral, FL, where we walk through diagnostic workup, layered medical protocols, and procedural options matched to your Fitzpatrick category and active acne severity.
Frequently Asked Questions
1. Is acne treatment really different on dark skin?
Yes. The acne lesion is similar, the pigmentary response is not. Acne in skin of color leaves dark marks more readily, lasts longer, and responds differently to aggressive treatment. Standard protocols designed for Fitzpatrick II skin frequently make pigmentation worse.
2. Why does my acne leave dark spots that last for months?
Post-inflammatory hyperpigmentation is the result of melanocyte activation during inflammation. In Fitzpatrick III to VI skin, melanocytes deposit pigment that takes months to fade. Sun exposure deepens it. Daily mineral sunscreen is essential, and pigment-targeted ingredients accelerate the fade.
3. Can I use benzoyl peroxide if I have dark skin?
Yes, but as a targeted spot treatment rather than an all-over wash. Benzoyl peroxide dark skin protocols emphasize lower concentrations and shorter contact time. Salicylic acid is usually a better daily baseline.
4. Is azelaic acid safe for dark skin?
Yes. Azelaic acid for dark skin is one of the safest active ingredients available and one of the few that addresses both acne and pigment at once without increasing PIH risk.
5. Do I need a dermatologist or can a medical aesthetics clinic treat this?
A medical aesthetics clinic like Perfect B can handle most acne presentations in Fitzpatrick III to VI skin, including in-office procedures, topical protocols, and PIH management. For very severe cases that may require systemic medication, we coordinate with a dermatologist.
6. How long until I see results on a properly designed protocol?
Active acne typically improves visibly within 4 to 6 weeks on the layered protocol. Dark marks from previous lesions fade over 3 to 12 months depending on depth and consistency with sunscreen and pigment care.
7. Do you treat dark skin acne at Perfect B in Doral?
Yes. Our Doral, FL clinic serves a heavily Fitzpatrick III to VI patient base, reflecting the Hispanic and Latin demographics of South Florida. Every protocol we build is calibrated to your Fitzpatrick category and current barrier status. Book a consultation and our medical team will map the right approach for your skin.
Closing: The Clinical Bottom Line on Dark Skin Acne Treatment
Dark skin acne treatment in Miami is fundamentally about pigment management as much as acne management. The protocol that clears a Fitzpatrick II patient in 4 weeks can leave a Fitzpatrick V patient with dark marks for a year. Recognizing that biological difference is the start of every good clinical decision.
What separates clinic-supervised care from a drugstore routine is not the ingredient list. Both have access to salicylic acid, azelaic acid, niacinamide, and sunscreen. What changes is the sequencing, the dose calibration, the procedural escalation when home care plateaus, and the willingness to slow down when the skin signals stress. That clinical judgment is the difference between clear skin in 8 weeks and a year of dark marks chasing each other.
- 📍 Visit us at Perfect B | 3905 NW 107th Ave, Suite 104, Doral FL 33178
- 📞 Call or message us at (786) 502-2260
- 💳 Buy Now Pay Later available: Cherry, Klarna, Afterpay, CareCredit


