

Perfect B, Doral Fl. | 04.29.26 | 8 min read.
This content is for educational purposes only and does not constitute medical advice. Peptide therapies should be prescribed and supervised by a licensed medical provider. Individual results vary.
Key Takeaways: What Tesamorelin Actually Does to Appetite and Body Composition
- Tesamorelin does not directly suppress appetite. Patients at Perfect B do not typically report reduced hunger. That effect belongs to GLP-1 medications like semaglutide and tirzepatide.
- Any appetite change is secondary. As sleep, recovery, and body composition improve on tesamorelin, patients naturally feel more motivated to eat well. The peptide changes the conditions, not the hunger signal itself.
- Tesamorelin is the most evidence-backed peptide for reducing abdominal visceral fat, more so than CJC-1295/Ipamorelin or AOD 9604.
- The timeline is gradual: better sleep and energy at 4 weeks, less bloating and improved recovery at 8 weeks, measurable body composition changes by 12 weeks.
- InBody scans often lag behind what patients feel. Visible waist changes and reduced bloating appear before the numbers on a scan shift significantly.

Does Tesamorelin Actually Suppress Appetite?
The short answer is no, not directly. Patients at Perfect B who start tesamorelin do not typically report a reduction in hunger. This surprises people who have read about it in the context of fat loss and assumed it would work the same way GLP-1 medications do.
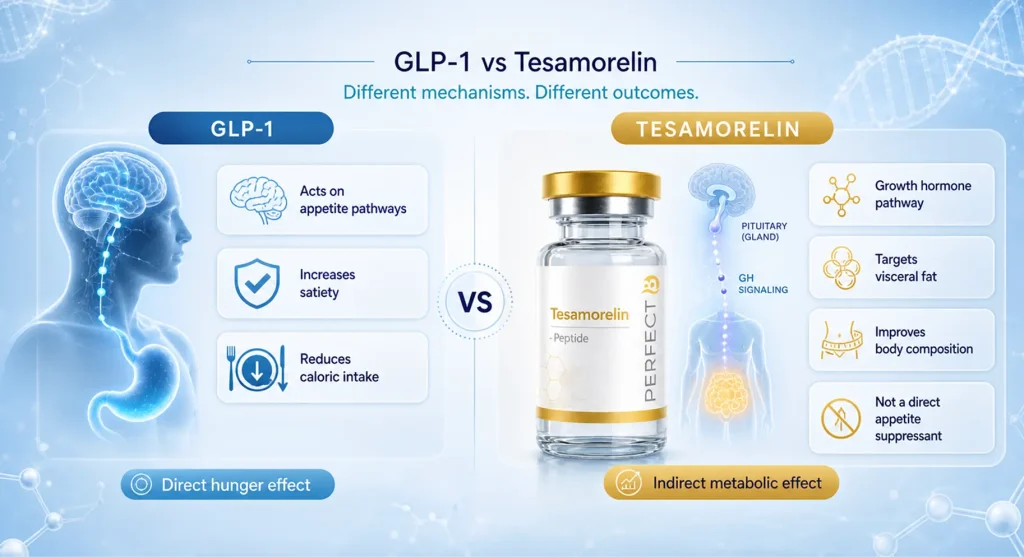
GLP-1 medications, specifically semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound), work in part by acting on receptors in the brain that regulate hunger. The appetite suppression with those medications is direct and often significant. Patients report reduced cravings, smaller portion sizes, and a general disinterest in food they previously found compelling.
Tesamorelin does not operate through that mechanism. It is a growth hormone-releasing factor analogue. It stimulates the pituitary gland to produce more of your own growth hormone. That increase in growth hormone is what drives the metabolic and body composition changes the peptide is known for. Appetite regulation is not part of that pathway.
Why Patients Sometimes Feel Like Their Appetite Has Changed
This is where the clinical picture gets more nuanced. Some patients do report eating differently after several weeks on tesamorelin, and they are not wrong to notice it. The shift is real. But the mechanism is secondary, not direct.
As tesamorelin improves sleep quality, energy levels, and overall recovery, patients start feeling better in a general sense. When someone is sleeping well, has more energy during the day, and feels like their body is responding to effort again, they tend to make better food choices. The motivation to eat well follows from the physical improvement, rather than the peptide suppressing hunger signals directly.
At our clinic in Doral, FL, we explain this distinction clearly at the start of every tesamorelin protocol. Patients who come in expecting appetite suppression similar to semaglutide will be disappointed if they do not understand what tesamorelin is actually doing. The ones who see the best results are those who use the improved sleep and energy as a foundation to build better habits around, not those waiting for a drug to remove hunger from the equation.
How Tesamorelin Compares to CJC-1295/Ipamorelin and AOD 9604 for Fat Loss
Patients often ask how tesamorelin stacks up against other peptides they have read about. The three that come up most are CJC-1295/Ipamorelin and AOD 9604. All three affect fat in some way, but they work differently and are not interchangeable.
Tesamorelin: Targeted Visceral Fat Reduction
Tesamorelin has the strongest published evidence for reducing abdominal visceral fat specifically. The clinical trials that led to FDA approval demonstrated consistent reductions in visceral adipose tissue, measured by imaging. Peer-reviewed research on tesamorelin consistently confirms its mechanism as a growth hormone secretagogue with targeted effects on visceral adiposity, making it distinct from general fat loss agents. If the primary goal is reducing the hard belly fat that sits around the organs, tesamorelin is the most evidence-backed option available. The FDA drug information page for tesamorelin confirms its approved clinical indication and provides prescribing context for medical providers and patients.
CJC-1295/Ipamorelin: Lean Muscle as the Primary Driver
CJC-1295/Ipamorelin also works by increasing growth hormone output, but its clinical application is more focused on building lean muscle mass. Patients who are primarily interested in improving body composition through muscle gain, enhancing sleep quality and recovery, and seeing overall anti-aging effects tend to be better served by CJC/Ipamorelin. Some fat loss occurs as a secondary benefit, but it is not the primary mechanism. Our complete guide to CJC-1295/Ipamorelin covers how this growth hormone stack works, who it is for, and what patients at Perfect B actually experience on it.
AOD 9604: Fat Metabolism Without the Muscle and Recovery Effects
AOD 9604 targets fat metabolism more directly than either of the above, but the evidence base for visceral fat specifically is thinner than what exists for tesamorelin. It does not carry the same muscle-building and recovery benefits. For patients with a very specific goal of fat metabolism support, it can be a useful tool, but it is not a replacement for tesamorelin when visceral fat reduction is the clinical objective.

The Tesamorelin Timeline: What Actually Changes at 4, 8, and 12 Weeks
One of the most important things we tell patients before starting tesamorelin is that the results follow a specific sequence. Understanding that sequence prevents the frustration that comes from expecting body composition changes in the first month.
Around Week 4: Sleep and Energy
The first changes patients reliably report are improvements in sleep quality and overall energy. They are sleeping more deeply, waking up feeling more rested, and noticing more consistent energy through the day. This is the growth hormone effect working on recovery and sleep architecture. At this stage, the scale has not moved and the InBody scan looks the same. Patients who were not prepared for this tend to question whether the peptide is working. It is working.
Around Week 8: Bloating and Recovery
By the two-month mark, patients start noticing less bloating and a faster recovery from physical activity. The belly that felt chronically distended begins to look and feel different. This is not yet body composition change in the way a scan would capture it. It is the early metabolic shift, with the visceral fat beginning to respond and the inflammation that surrounds it starting to reduce.
Around Week 12: Body Composition
The twelve-week mark is when measurable changes in body composition typically emerge: increased lean muscle mass, a decrease in visceral fat, and visible changes to waist circumference and overall shape. This is the target outcome, and it takes three full cycles to get there consistently. Patients who stop at eight weeks because they are not seeing dramatic scan results are stopping right before the payoff phase.

Who Is the Right Candidate for Tesamorelin?
Tesamorelin is not a universal fat loss tool. It performs best for a specific patient profile, and being honest about that profile is part of how we get good results at Perfect B.
The patients who respond best to tesamorelin share several characteristics:
- High visceral fat: The stubborn abdominal fat that sits deep around the organs, not subcutaneous fat just under the skin. Tesamorelin’s mechanism is specifically targeted at this type.
- Insulin resistance: Patients with metabolic dysfunction, including pre-diabetes or difficulty managing blood sugar, tend to see meaningful improvement in metabolic markers alongside body composition changes.
- Stubborn belly fat despite diet and exercise: Patients who are doing the right things but finding that their midsection does not respond. This is often driven by the visceral fat component rather than caloric excess.
- Low lean muscle mass: Tesamorelin’s growth hormone stimulation supports muscle preservation and growth alongside fat reduction, making it useful for patients who are losing both.
- Willingness to be consistent and build habits: Tesamorelin is not a shortcut. The patients who see the best results are those who pair it with improved nutrition, regular movement, and the sleep improvements the peptide helps create.
Who Tesamorelin Is Not the Right Fit For
This is a question we take seriously at our Doral clinic, because prescribing a peptide to a patient whose goals do not match the mechanism is a setup for disappointment.
Tesamorelin is not the right choice for patients who:
- Want appetite suppression or reduced cravings: That effect belongs to GLP-1 medications. Tesamorelin will not reliably curb hunger, and patients expecting that effect will not get it.
- Are primarily trying to lose weight on the scale: Tesamorelin shifts body composition. Patients can see their waist change, their shape improve, and their visceral fat reduce while the number on the scale moves very little. If the goal is scale weight, this is not the right tool.
- Only need to increase lean muscle mass: CJC-1295/Ipamorelin is more targeted for that goal and may be a better fit.
- Are not willing to make lifestyle changes: Tesamorelin creates better conditions. It does not override poor sleep, sedentary habits, or a diet that defeats its metabolic effects. Patients who expect the peptide to do all the work consistently underperform.
Choosing the right peptide for the right goal is what separates a protocol that works from one that frustrates. Our full breakdown of what tesamorelin is, how it works at the molecular level, and what the FDA approval data actually shows covers the mechanism in depth for patients who want the full picture before deciding.
What the InBody Scan Shows in the First Three Cycles: What It Misses
One of the more clinically interesting patterns we see with tesamorelin at Perfect B is the disconnect between how patients feel and what the InBody scan shows in the first three cycles.
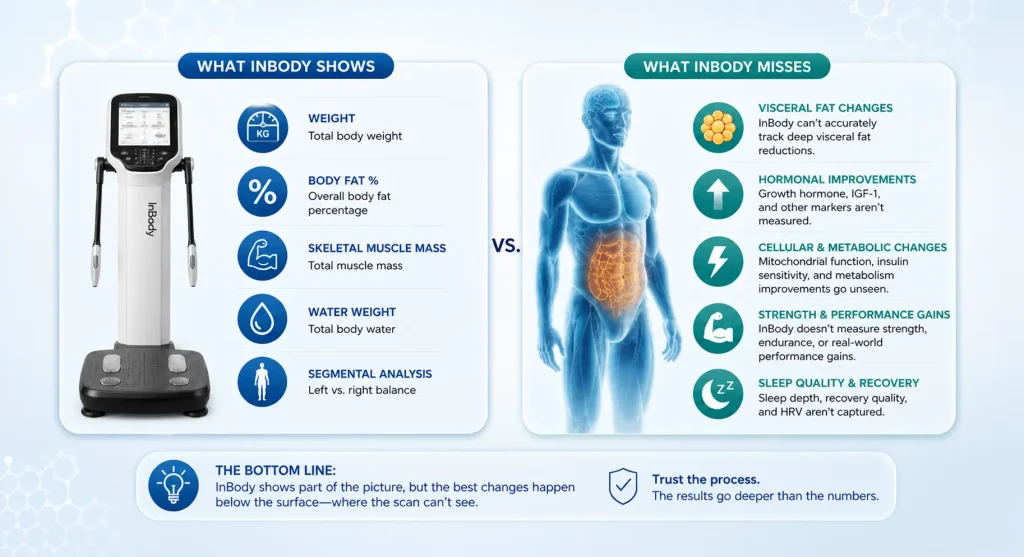
InBody scans measure segmental body composition: lean mass, fat mass, and fluid distribution. They are useful tools, but they capture a snapshot of tissue-level data that lags behind what the patient experiences. In the first three cycles of tesamorelin, dramatic changes on the scan are not the norm. Patients who judge their progress entirely by the scan numbers at week 12 often conclude the treatment is not working.
What those same patients report subjectively tells a different story. Their waist is smaller. Clothes fit differently. The bloating they had accepted as normal is gone. Their shape has shifted even when the total fat mass number on the scan has not moved as much as expected. These are real, measurable changes in visceral fat that a surface-level scan captures imperfectly, especially in the early cycles.
We use the InBody as one data point, not the definitive verdict on tesamorelin’s effectiveness. Clinical observation, waist circumference, and patient-reported changes across sleep, energy, and recovery give a more complete picture of how the protocol is actually working. The scan numbers tend to catch up as the protocol continues past the initial three cycles. Our detailed dosage guide at our tesamorelin dosage and injection protocol page covers cycle length, how we structure ongoing treatment, and what to track between appointments.
Tesamorelin vs GLP-1 Medications: Different Tools for Different Problems
Patients frequently come in having used or considered semaglutide or tirzepatide and want to know how tesamorelin compares. The honest answer is that they are not competing tools. They address different underlying problems.
GLP-1 medications work by mimicking the GLP-1 hormone, which slows gastric emptying, signals satiety to the brain, and helps regulate blood sugar. The weight loss is driven substantially by appetite suppression and reduced caloric intake. For patients with obesity, type 2 diabetes, or significant metabolic syndrome, GLP-1 medications have strong evidence and meaningful clinical outcomes.
Tesamorelin works by stimulating growth hormone production. It does not touch the appetite pathway. Its strength is in shifting body composition from the inside: reducing visceral fat, improving lean muscle mass, and restoring metabolic function that has declined with age or hormonal changes. For patients in the Miami area who are not candidates for GLP-1 medications, or who have already used them and want to address the body composition residue that appetite suppression alone does not fix, tesamorelin fills a gap those medications leave.
In some protocols, they are used together, with each addressing the part of the problem the other does not reach. That decision is made in consultation, based on the individual patient’s labs, history, and goals.
Frequently Asked Questions
1. Does tesamorelin suppress appetite?
Not directly. Patients at Perfect B do not typically report reduced hunger on tesamorelin. Any appetite-related changes are secondary: as sleep improves, energy returns, and body composition shifts, patients naturally feel more motivated to support those changes with better nutrition. Direct appetite suppression is a GLP-1 mechanism, not a growth hormone mechanism.
2. How long does tesamorelin take to work?
The effects follow a sequence. Most patients notice improved sleep and energy by week 4. Reduced bloating and faster recovery appear around week 8. Measurable body composition changes, including decreased visceral fat and increased lean muscle, emerge around week 12. InBody scan numbers often lag behind what patients feel physically.
3. Can tesamorelin be stacked with other peptides for better fat loss?
Yes. Tesamorelin is commonly used alongside other peptides when the clinical picture calls for it. The specific combination depends on the patient’s goals. Someone needing both visceral fat reduction and lean muscle building might use tesamorelin alongside CJC-1295/Ipamorelin. Those decisions are made based on labs and a clinical consultation, not a general protocol.
4. Who is a good candidate for tesamorelin at Perfect B?
Patients with high visceral fat, insulin resistance, stubborn abdominal fat that does not respond to diet and exercise, and low lean muscle mass tend to respond best. Consistency and a willingness to build healthy habits alongside the protocol are also factors in outcomes. Tesamorelin is not well-suited for patients whose primary goal is appetite suppression or scale weight loss.
5. What side effects do patients actually experience on tesamorelin?
The most commonly reported side effect is mild injection site irritation in the early weeks, which typically resolves. Some patients notice mild water retention or joint discomfort early in the protocol as growth hormone levels adjust. These effects are transient. Serious adverse events are rare, particularly when the peptide is prescribed and monitored by a licensed provider with appropriate lab work.
6. Is tesamorelin only for visceral fat, or does it help with overall weight loss?
Tesamorelin’s strongest evidence is for visceral fat specifically, which is the metabolically active fat that surrounds organs in the abdominal cavity. Overall scale weight may not change dramatically because lean muscle mass tends to increase alongside fat reduction. The body composition shift is the goal, not the number on the scale.
7. How is tesamorelin different from semaglutide or tirzepatide?
Entirely different mechanisms. GLP-1 medications suppress appetite and regulate blood sugar by mimicking the GLP-1 hormone. Tesamorelin stimulates growth hormone production via the pituitary gland and does not touch the appetite pathway. GLP-1 medications drive weight loss primarily through reduced caloric intake. Tesamorelin drives body composition changes through metabolic and hormonal shifts. They address different problems and are sometimes used together in the same patient.
Closing: The Right Expectation Makes All the Difference
Tesamorelin does not suppress appetite. Patients who start the protocol expecting hunger to disappear will be disappointed at week four. Patients who understand that the peptide is rebuilding the metabolic foundation, starting with sleep and energy, progressing through recovery and bloating, and arriving at body composition changes by week twelve, tend to stay the course and see results that match what the research shows. The timeline is not a bug. It is the mechanism.
At Perfect B in Doral, FL, our approach to tesamorelin is grounded in clinical honesty: the right peptide for the right patient, with realistic timelines and the monitoring to catch what a self-administered protocol cannot. If your goal is reducing visceral fat, improving body composition, and restoring the metabolic function that changes with age, tesamorelin is worth a serious conversation. If your goal is appetite suppression, we can help you understand which tool actually does that.
📍 Visit us at Perfect B, 8200 NW 41st St Suite 100, Doral, FL 33166
📞 Call or message us at (786) 502-2260


