

Perfect B, Doral FL. | 05.08.26 | 9 min read.
This post is for educational purposes only and does not substitute for personalized medical advice. Retinoid protocols vary based on skin type, sensitivity, and clinical history. Consult a licensed medical provider before beginning any prescription retinoid treatment.
What Makes Something a Retinoid and Why It Matters
Retinoids are a family of compounds derived from vitamin A. The reason they are so widely used in dermatology and aesthetic medicine is that vitamin A receptors are present throughout the skin, and activating them triggers cellular processes that would otherwise slow down with age and sun damage: collagen production, cell turnover, pigment regulation, and sebaceous gland activity. That is a short description of why this class of ingredients addresses such a wide range of concerns, from acne to wrinkles to dark spots.
The confusion arises because retinoid is not a single ingredient. Retinol, adapalene, and tretinoin are all retinoids. They are not interchangeable. They differ in potency, mechanism, availability, and the conditions they are best suited to treat. Choosing the wrong one does not necessarily cause harm, but it often means slower results, unnecessary irritation, or treating one problem while neglecting another.
The vitamin A conversion chain
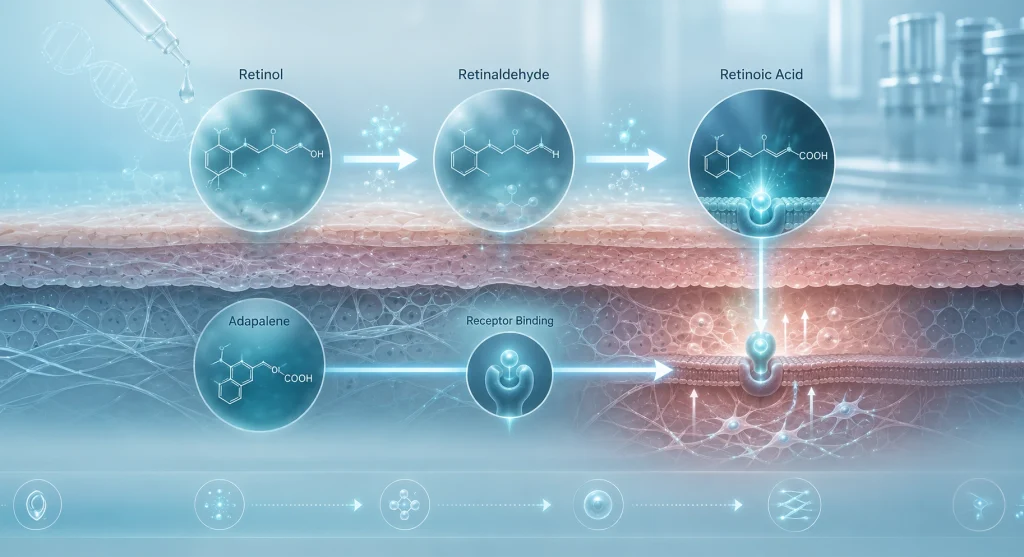
To understand why these three compounds perform differently, you need to understand how vitamin A works in skin. The active molecule that binds to skin receptors is retinoic acid. Tretinoin is retinoic acid, meaning it arrives at the receptor without requiring any conversion. Retinol must be converted in the skin through two enzymatic steps: retinol to retinaldehyde, then retinaldehyde to retinoic acid. That conversion process is enzymatic, variable, and inefficient. Two people applying the same retinol 1% serum will produce different amounts of retinoic acid in their skin depending on their individual enzyme activity. Adapalene is a synthetic third-generation retinoid that binds selectively to specific retinoic acid receptors without requiring conversion. It is not retinoic acid itself, but it acts more directly than retinol does.
Why bioavailability determines how fast results appear
This conversion chain explains the timeline differences between the three compounds. Tretinoin starts working at the receptor immediately. Adapalene reaches its target receptors directly via a specific binding pathway. Retinol takes longer to produce visible results not because it is weaker per se, but because less of what you apply actually becomes active at the receptor level. A systematic review published in the International Journal of Women’s Dermatology confirming that topical tretinoin consistently improved photoaging across all seven randomized controlled trials reviewed, covering wrinkles, mottled hyperpigmentation, and skin texture reflects the evidence base that no other retinoid can match at equivalent timelines.
Key Takeaways
- Tretinoin is the only retinoid with FDA approval for both acne and photoaging, and the only one that acts directly as retinoic acid without requiring enzymatic conversion in the skin.
- Adapalene is the OTC retinoid with the strongest clinical evidence for acne, as effective as tretinoin 0.025% for acne treatment in head-to-head trials but significantly less irritating.
- Retinol is best suited for prevention and maintenance, not active treatment. If you have acne or want to address real photoaging, retinol alone is usually insufficient.
- For Fitzpatrick III-V skin types, the order of introduction matters more because retinoid-induced irritation can trigger post-inflammatory hyperpigmentation. Adapalene is typically the safest entry point.
- The retinoid ladder is not mandatory. The right starting point depends on what you are treating, your skin’s baseline tolerance, and your provider’s assessment.
Retinol: The OTC Starting Point and Its Limitations
Retinol is the most widely available retinoid and the one most people encounter first. It is sold in serums, creams, and oils at concentrations ranging from 0.025% to 1%. The fact that it is over-the-counter and extensively marketed gives many patients the impression that it is a comprehensive retinoid solution. It is not.
Who retinol is actually right for
Retinol is appropriate for patients who want to begin retinoid use for prevention and general skin quality maintenance, who have mild concerns about early fine lines or uneven texture, who have sensitive skin and cannot tolerate stronger retinoids at the outset, or who are not dealing with active acne. At Perfect B, we use retinol-based formulations as a maintenance tool, particularly during periods when a patient needs to pause their tretinoin use, such as during increased sun exposure or when supporting the skin barrier after a clinical procedure.
The limitation of retinol is conversion variability. A well-formulated retinol 1% in a stable base will produce meaningful results over months of consistent use. But many OTC retinol products are poorly formulated: the retinol oxidizes quickly when exposed to air and light, leaving an ineffective product that the patient continues applying. A product that has changed color or odor is degraded retinol delivering far less than the label states.
Why the conversion process makes results unpredictable
The two-step enzymatic conversion from retinol to retinoic acid is not consistent across individuals. Patients with higher enzyme activity will convert more efficiently and see faster results. Those with lower activity will see slower results from the same product. This variability is the clinical reason we often move patients from OTC retinol to prescription retinoids when their goals are active treatment rather than maintenance. You cannot titrate an outcome you cannot control.
Adapalene: The OTC Retinoid That Changed the Access Equation
Adapalene is a third-generation synthetic retinoid that was, until 2016, available only by prescription in the United States. The FDA’s decision to approve Differin 0.1% gel as an over-the-counter product was a significant clinical access shift. Adapalene is now the only prescription-strength retinoid mechanism available without a prescription in the US, and it is the one we most commonly recommend as a first clinical retinoid for patients who need a retinoid for acne but are not yet ready for a prescription or who cannot access one easily.
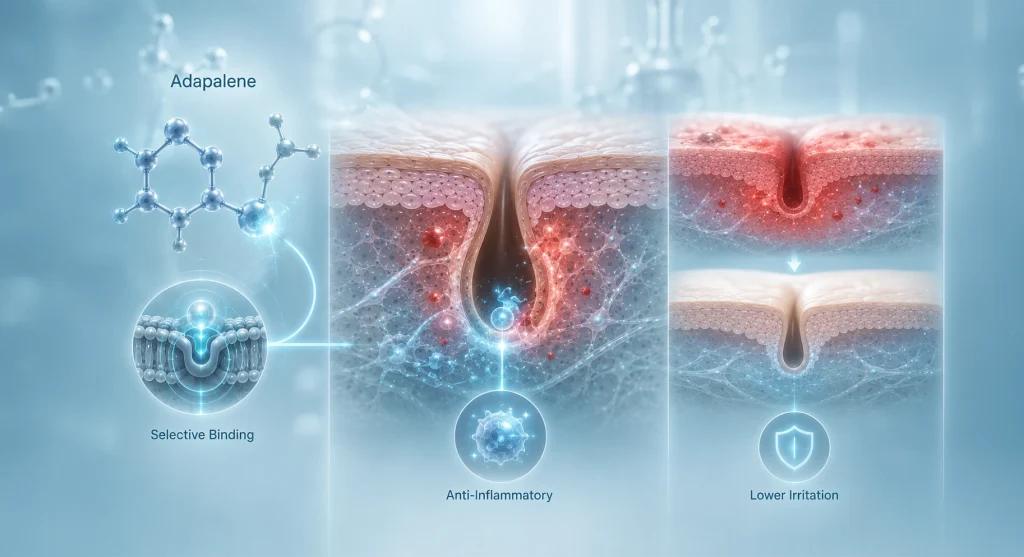
Why adapalene is the first clinical choice for acne
Adapalene’s mechanism is specific and well-suited to acne biology. It binds selectively to retinoic acid receptors RAR-beta and RAR-gamma, which are the receptors involved in keratinocyte differentiation and comedone formation. This selectivity produces potent anti-comedogenic and anti-inflammatory effects with less non-specific receptor activation, which is why it causes less irritation than tretinoin at equivalent acne-treating concentrations. A multicenter clinical trial published in the Journal of the American Academy of Dermatology confirming comparable efficacy between adapalene 0.1% and tretinoin 0.025% for acne vulgaris with significantly lower irritation in the adapalene group established the clinical basis for this approach.
Adapalene 0.1% gel is effective for comedonal and inflammatory acne. Clinical studies show meaningful lesion count reduction between 8 and 12 weeks of consistent use. For patients with moderate acne who want to start a retinoid without a provider visit, adapalene 0.1% is the evidence-based recommendation. For severe or persistent acne, adapalene alone is typically insufficient and a prescription retinoid or combination treatment is more appropriate. → See how Perfect B builds acne treatment plans in Doral, FL that integrate retinoids with clinical-grade interventions for patients who need more than OTC solutions.
Adapalene for anti-aging: what the evidence says
Adapalene’s anti-aging evidence is more limited than tretinoin’s but not absent. Studies at higher concentrations, specifically adapalene 0.3%, have shown comparable efficacy to tretinoin 0.05% for photoaging outcomes. At the OTC concentration of 0.1%, the anti-aging effects are meaningful but more gradual than tretinoin 0.025% for wrinkle improvement. If the primary goal is anti-aging rather than acne, adapalene 0.1% is a reasonable starting point but tretinoin is the more direct path for most patients.
Why adapalene is the safest entry retinoid for Fitzpatrick III-V skin
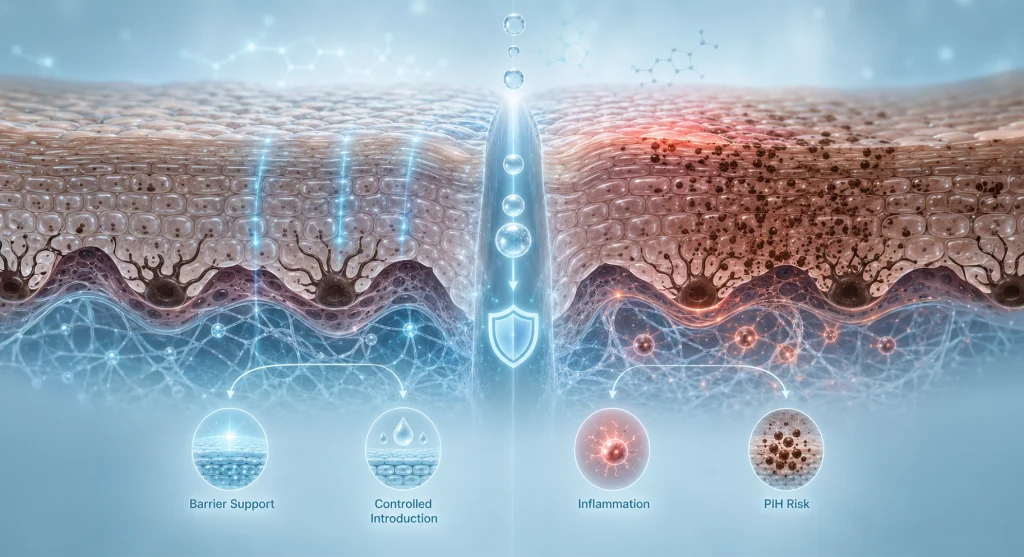
On melanin-rich skin, retinoid-induced irritation carries a risk that does not apply to Fitzpatrick I-II patients: post-inflammatory hyperpigmentation. When the skin becomes irritated or damaged from over-application of a retinoid, the melanocytes respond by producing excess pigment at the site of inflammation. In patients with Fitzpatrick III, IV, and V skin, this response is more pronounced and more persistent. The result can be dark marks that take months to fade, replacing one skin concern with another.
Adapalene’s lower irritation profile makes it a safer first retinoid for our patient population in Doral, where a high proportion of patients present with Latin American, Hispanic, and Caribbean skin types. Starting with adapalene allows the skin to adapt to retinoid use, and if the patient tolerates it well and needs more potency, we can transition to tretinoin with a skin barrier that has already been conditioned. → Learn how Perfect B tailors skincare treatment plans in Doral, FL for South Florida skin types, including Fitzpatrick-specific retinoid protocols.
Tretinoin: The Prescription Standard and Why It Earns That Status
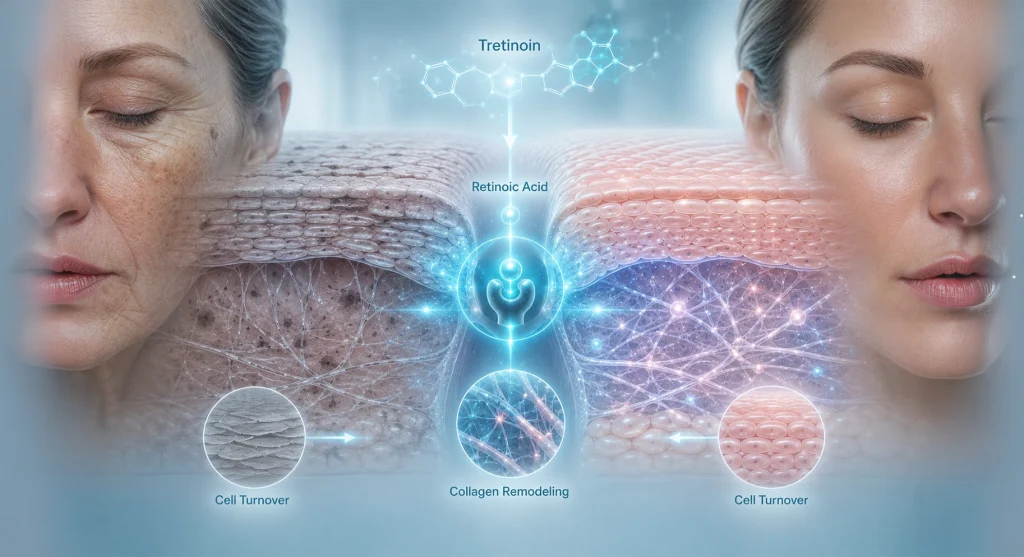
Tretinoin is retinoic acid. It is the end product of the vitamin A conversion chain, delivered directly to the skin’s retinoid receptors without any intermediate steps. It is available only by prescription at concentrations ranging from 0.01% to 0.1%, and it is the most extensively studied topical retinoid in clinical literature. The body of evidence for tretinoin spans over five decades and covers acne, photoaging, pigmentation, and skin texture. No other topical retinoid has a comparable evidence base.
What tretinoin does that retinol and adapalene cannot match
Tretinoin’s direct receptor binding produces outcomes that neither retinol nor adapalene can replicate at equivalent timelines. For photoaging specifically, tretinoin is the only retinoid with FDA approval to treat fine lines, wrinkles, and mottled hyperpigmentation from sun damage. It stimulates collagen type I production more robustly than adapalene. It normalizes cell turnover more completely than retinol. For patients whose goals include significant improvement in photoaged skin, acne scarring, or deep textural irregularity, tretinoin is the clinical standard.
Tretinoin for acne scars, dark spots, and photoaging
In acne scar management at Perfect B, tretinoin is a component of our maintenance protocol after clinical procedures. Once the active acne is controlled and scar treatments like microneedling or TCA Cross have been completed, tretinoin maintains the cellular turnover gains and continues the collagen remodeling process between sessions. For post-acne dark spots, tretinoin’s acceleration of cell turnover progressively brings pigmented cells to the surface where they shed. For photoaging, the collagen stimulation and normalization of epidermal architecture produce improvements in skin texture and tone that accumulate over months of consistent use.
The purge: what to expect and when to push through
Tretinoin causes a purging phase in most patients that begins within the first two to four weeks of use and can last six to ten weeks. The purge happens because tretinoin accelerates cell turnover, bringing microcomedones that were forming below the surface to the skin surface faster than they would have emerged on their own. The breakouts are not new acne caused by tretinoin. They are existing acne being expelled more rapidly. Patients who stop tretinoin during the purge phase often conclude it does not work for them, when in fact they quit precisely when the mechanism was functioning correctly. → Read Perfect B’s complete guide to the tretinoin purge in Doral, FL, including what to expect week by week and when to call your provider.
The Retinoid Ladder: How Perfect B Approaches the Progression
The retinoid ladder is a clinical framework that starts with the least potent, least irritating retinoid and escalates based on tolerance and clinical need. It is a useful guide but not a rule. Not every patient needs to start at the bottom. Someone presenting with moderate persistent acne who has never used any retinoid does not need to spend three months on retinol before being prescribed adapalene. The ladder is a decision framework, not a mandatory sequence.
At Perfect B, the starting point is determined by three variables: what the patient is treating, their baseline skin sensitivity, and their Fitzpatrick type. For a Fitzpatrick II patient with mild fine lines and no active acne, we may go directly to adapalene for more reliable results. For a Fitzpatrick IV patient with active acne and minimal retinoid experience, we start with adapalene to build tolerance before considering tretinoin. For a patient with significant photoaging or acne scarring who needs real clinical change in a defined timeline, we start with tretinoin at a low concentration and titrate up. The question we ask is not what is the safest option in isolation, but what is the right tool for this patient’s biology and this patient’s goals at this moment.
Fitzpatrick III-V and Why Skin Tone Changes the Retinoid Protocol
For patients with Fitzpatrick I-II skin, the primary concern with retinoids is irritation and the temporary redness and peeling of the adjustment phase. For patients with Fitzpatrick III-V skin, there is an additional variable: the risk that irritation-induced inflammation triggers post-inflammatory hyperpigmentation. The skin does not just peel and recover in the same way. It may produce excess melanin at the irritation site, creating dark marks that persist for months.
This does not mean darker skin types cannot use tretinoin. It means the protocol needs to account for this risk. At Perfect B, our approach for Fitzpatrick IV-V patients beginning retinoid therapy includes starting at the lowest effective concentration, applying every other night initially rather than nightly, using a barrier-supportive moisturizer before and after application if needed, avoiding concurrent use of other active ingredients during the adjustment phase, and pairing with a broad-spectrum mineral sunscreen every morning without exception.
Using Retinoids in Miami: Sun Exposure and What to Do Differently
Every retinoid increases photosensitivity. This is not a minor consideration in a city where the UV index regularly reaches the highest levels in the continental United States and where patients spend meaningful time outdoors year-round. The Miami context means the standard use sunscreen with retinoids instruction is not enough.
Our specific guidance for Doral and Miami patients on retinoid protocols: apply retinoids at night only, never during the day. Use a broad-spectrum mineral sunscreen SPF 30 or higher every morning without exception, regardless of whether outdoor time is planned. Avoid prolonged midday sun exposure during the first eight weeks of a new retinoid, when photosensitivity is highest. If a beach day or extended sun exposure is unavoidable, skip the retinoid application the night before and the night after. The combination of active retinoid use and Miami-level UV exposure without consistent protection is one of the most reliable ways to develop retinoid-induced hyperpigmentation, particularly on Fitzpatrick III-V skin.
Frequently Asked Questions
1. Is tretinoin stronger than retinol?
Yes, significantly. Tretinoin is retinoic acid, the active molecule that directly binds to skin receptors. Retinol must be converted through two enzymatic steps before becoming active, and that conversion is variable and inefficient. At equivalent concentrations on the label, tretinoin is substantially more potent and produces results faster and more predictably.
2. Can I buy tretinoin without a prescription?
No. Tretinoin requires a prescription in the United States. If you are looking for an OTC option with real clinical evidence, adapalene 0.1% (sold as Differin) became available without a prescription in 2016 and is the strongest retinoid mechanism accessible without a provider visit. For tretinoin, a medical consultation is required.
3. Is adapalene as good as tretinoin for acne?
For acne, yes at comparable concentrations. Head-to-head clinical trials show adapalene 0.1% and tretinoin 0.025% produce similar lesion count reductions for acne vulgaris, with adapalene causing significantly less irritation. For anti-aging and photoaging, tretinoin has stronger evidence and produces more robust collagen stimulation. The choice depends on whether acne or aging is the primary concern.
4. Can I use tretinoin if I have dark skin?
Yes, with the right protocol. Darker skin types can use tretinoin, but the approach needs to account for the higher risk of post-inflammatory hyperpigmentation that comes with retinoid-induced irritation. At Perfect B, we often start Fitzpatrick IV-V patients on adapalene to build tolerance before transitioning to tretinoin, and we use conservative starting concentrations and application frequencies when beginning tretinoin directly.
5. How long does tretinoin take to work?
Most patients see meaningful improvement in acne within 8 to 12 weeks of consistent use, after the purge phase resolves. Anti-aging benefits including improvements in fine lines, skin texture, and pigmentation develop more gradually, with noticeable results typically visible at 3 to 6 months of consistent nightly use. Full collagen remodeling continues to develop over 12 months or more.
6. Can I use retinol and adapalene at the same time?
This is not typically recommended. Both are retinoids and using them together increases the risk of irritation without meaningfully increasing efficacy. Choose one based on your primary concern and use it consistently. If you are using adapalene for acne and want to introduce anti-aging benefits, your provider can advise whether transitioning to tretinoin makes more sense for your skin.
7. What should I use with a retinoid to minimize irritation?
A gentle non-foaming cleanser, a fragrance-free moisturizer with ceramides or hyaluronic acid, and a broad-spectrum mineral sunscreen used every morning are the core supporting products for any retinoid protocol. Avoid AHA or BHA exfoliants on the same nights as your retinoid during the first two months. Niacinamide is well tolerated alongside most retinoids and can help manage the initial redness and irritation of the adjustment phase.
Closing: The Right Retinoid Is the One Matched to Your Actual Skin
Retinoids are among the most evidence-supported tools in skin care. But the conversation about which one to use is often reduced to a potency ranking that treats adapalene and retinol as stepping stones toward tretinoin, as if tretinoin were the destination for everyone. It is not. For some patients, adapalene is the right long-term answer. For others, a well-formulated retinol is appropriate. For patients with active acne scarring, significant photoaging, or persistent hyperpigmentation, tretinoin is where the clinical impact is.
At Perfect B in Doral, FL, the retinoid conversation starts with your skin, your concerns, and your Fitzpatrick type. We look at what you are trying to treat, what your skin’s baseline tolerance looks like, and what level of intervention the evidence supports for your situation. → Book a consultation at Perfect B in Doral, FL to get a retinoid recommendation matched to your biology, your goals, and your skin type.
📍 Visit us at Perfect B, Doral FL
📞 Call or message us at (786) 502-2260


