

Perfect B, Doral FL. | 05.05.26 | 11 min read.
This content is for educational purposes only and does not constitute medical advice. Consult a qualified medical provider before beginning any acne treatment protocol. All treatments referenced on this page require a clinical evaluation from a licensed provider. Results vary by patient.
How to Cure Hormonal Acne: Why the Problem Is Never on the Surface
Knowing how to cure hormonal acne starts with understanding that it is a hormonal problem, not a skincare problem. Many patients arrive at Perfect B having spent months or years on hormonal acne natural treatments, over-the-counter products, and self-directed protocols that produced minimal or inconsistent results. The reason is not that these approaches are without value. It is that they address the symptom without touching the driver. Hormonal acne how to cure it properly means identifying the specific androgen pattern behind it, building a protocol around that data, and managing both the active breakouts and the damage they leave behind. At Perfect B in Doral, FL, when a patient sits down with those deep, painful cysts lining the jaw and chin, the first questions are not about products. They are about labs. Free and total testosterone, DHEA-S, cortisol, insulin, and vitamin D. Those numbers tell us more about your acne in one panel than a year of over-the-counter treatments ever could.
Key Takeaways
- Hormonal acne is driven by internal androgen activity: No topical product addresses the root trigger. Cleansing harder, layering more products, or switching brands does not change what is happening at the hormonal level.
- The labs most patients have never had: Free and total testosterone, DHEA-S, cortisol, fasting insulin, and vitamin D are the markers that reveal what is actually driving your breakouts. Most patients arrive at Perfect B having never had these tested.
- Spironolactone is currently first-line for adult women: Clinical data presented at the 2026 American Academy of Dermatology Annual Meeting confirmed spironolactone as one of the most effective systemic treatments for women with hormonal acne, as effective or more effective than oral antibiotics without the resistance risk.
- Miami adds a specific environmental layer: Heat, humidity, sweating, lifestyle stress, and cortisol elevation create conditions that worsen hormonal breakouts and require protocol adjustments specific to South Florida patients.
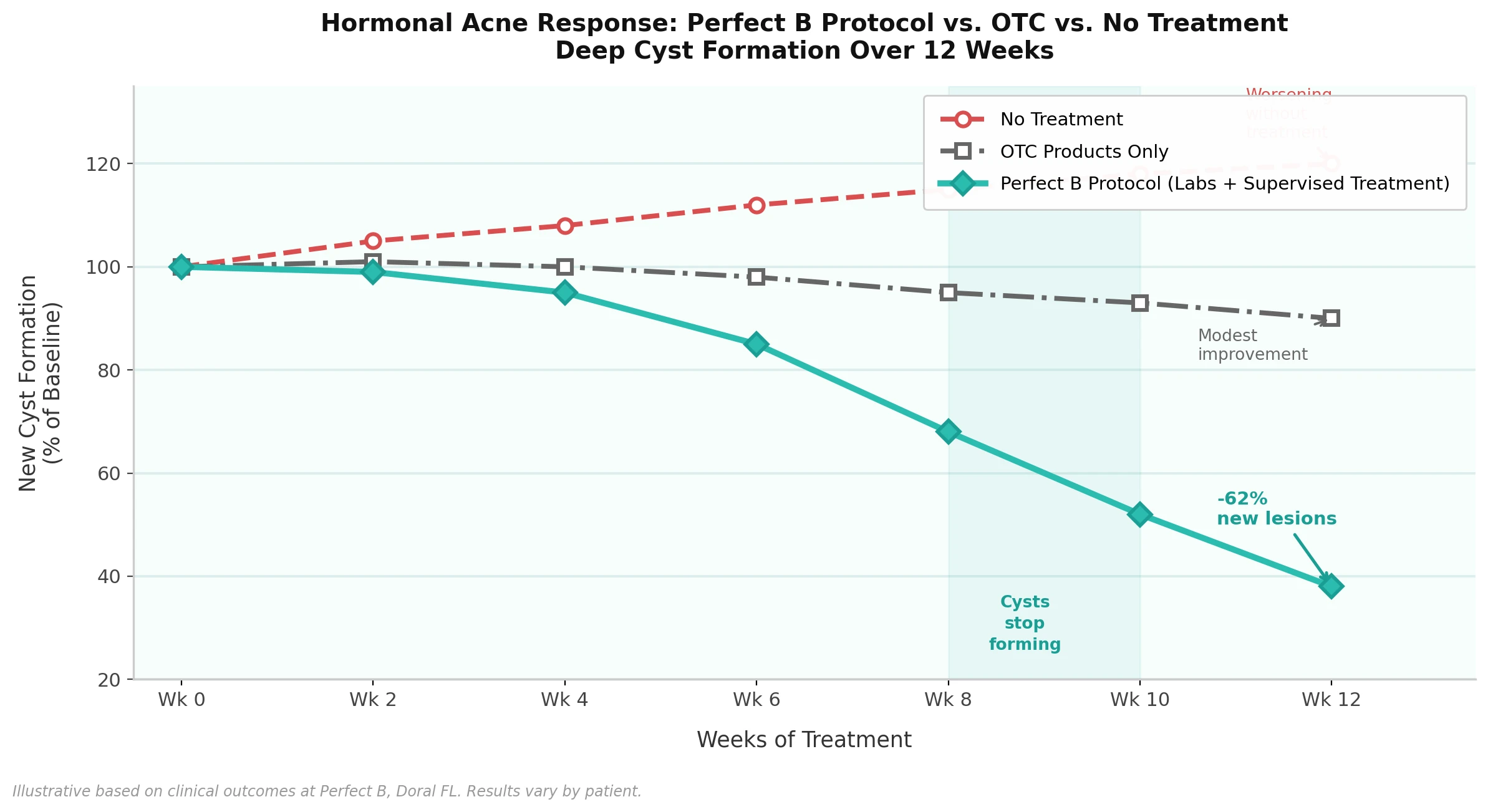
- 90 days is the first milestone, not the finish line: Within 90 days of a properly supervised protocol, the deep cysts stop forming. The skin is not flawless yet, but it is quiet. That silence is the foundation for everything that comes next.
What Is Hormonal Acne and How Do You Know If Yours Is Hormonal?
Hormonal acne is adult-onset acne driven by fluctuations in androgens, primarily testosterone and DHEA-S, which increase sebum production and trigger deep inflammation in the skin. Unlike adolescent acne, which typically appears across the forehead and nose as part of puberty, hormonal acne in adults concentrates along the jawline, chin, and lower cheeks. It presents as deep, painful nodules and cysts rather than surface-level blackheads or whiteheads, and it follows a pattern tied to internal hormonal shifts rather than random external triggers.
The clearest diagnostic signal is a predictable pattern. Breakouts that flare consistently the week before your period, worsen during high-stress periods, or appear in the same locations cycle after cycle are not a product problem. They are a hormonal signal. Other common patterns include acne that developed or worsened after stopping birth control, postpartum acne that persists beyond the expected recovery window, adult-onset acne appearing for the first time in the late 30s or 40s alongside other hormonal shifts, and breakouts that accompany PCOS symptoms such as irregular cycles, excess hair growth, or unexplained weight changes. Identifying the pattern is the first clinical step. Running the labs is the second.
The Labs That Reveal What Is Actually Driving Your Breakouts
The number of women walking around with high DHEA-S or rock-bottom vitamin D is striking, and in most cases nobody checked before. That is the adrenal androgen trigger hiding in plain sight. At Perfect B, the hormonal acne workup includes free and total testosterone, DHEA-S, cortisol, fasting insulin, and vitamin D. Each marker tells a different part of the story.
Free and total testosterone is the most direct driver of excess sebum production. When free testosterone is elevated, sebaceous glands produce more oil than the skin can manage, which creates the environment where cysts form. DHEA-S is an adrenal androgen that most general providers do not include in a standard hormonal panel. Elevated DHEA-S points to adrenal androgen excess rather than ovarian androgen excess, which changes the treatment approach significantly. Cortisol connects the stress-acne relationship with measurable data. Chronic cortisol elevation increases sebum production, impairs skin barrier function, and amplifies the inflammatory response to clogged pores. Fasting insulin is essential for any patient whose diet includes high-glycemic foods or who has signs of insulin resistance, because hyperinsulinemia directly stimulates androgen production. Vitamin D is consistently low in patients with persistent inflammatory acne and is one of the markers most patients have never had checked. Its role as an immune regulator and anti-inflammatory agent makes it a relevant factor in how aggressively the skin responds to hormonal triggers.
This panel is not optional at Perfect B. It is the foundation of the protocol. Without knowing which marker is driving the breakouts, any treatment is a guess. With it, the protocol is targeted, the timeline is realistic, and the results are explainable. A 2016 review published in Clinical, Cosmetic and Investigational Dermatology by NIH detailing the molecular mechanisms by which androgens stimulate sebaceous glands and how anti-androgenic interventions interrupt that pathway provides the scientific foundation for why this workup matters before any treatment decision is made.

The Three Treatment Lanes Perfect B Uses for Hormonal Acne
Once the labs are in and the hormonal driver is identified, the protocol gets built around what the data shows. At Perfect B, hormonal acne treatment falls into three lanes, and the severity and timeline of the breakouts determine which lane or combination of lanes is appropriate for each patient.
Lane One: Custom Topical Protocols for Mild Cases
For patients with mild hormonal acne, meaning infrequent deep lesions with manageable inflammation and no significant scarring, a custom topical regimen built around the specific hormonal trigger is the starting point. This is not a standard drugstore protocol. It is a combination of prescription-strength retinoids, targeted actives, and barrier-supportive products calibrated to the patient’s skin type and sensitivity. What differentiates the Perfect B approach is that the topical protocol is informed by the labs, not selected generically.
Lane Two: Oral Spironolactone for Deep Jawline Cysts
For patients with deep, painful cysts concentrated along the jawline and chin that have not responded to topicals, oral spironolactone is the heavy hitter. Spironolactone is an anti-androgen that blocks androgen receptors in the skin, reduces sebum production through multiple molecular pathways, and addresses the hormonal driver directly rather than managing symptoms on the surface. It is appropriate for adult women and is not used in male patients due to its anti-androgenic mechanism. Most patients see meaningful improvement within two to four months, with maximum benefit typically reached by month six. The important clinical note is that the progesterone-only pill or mini-pill can worsen hormonal acne in some patients by increasing androgenic activity, which is something to flag if a patient is already on hormonal contraception when they present.
Lane Three: In-Office Procedures for Scarring and Pigmentation
Once active breakouts are under control, the work shifts to addressing the damage left behind. Chemical peels reduce post-inflammatory hyperpigmentation, improve skin texture, and accelerate the clearance of dark marks. Microneedling stimulates collagen remodeling in the deeper layers of the skin where atrophic scarring has formed. At Perfect B, these procedures are introduced once the hormonal component is stabilized rather than applied to skin that is still actively inflamed. Our complete guide to acne scar treatment in Miami covers which Perfect B procedures address each scar type, what the treatment sequence looks like, and what results are realistic across multiple sessions.
Spironolactone for Hormonal Acne: What It Does, Who It Is For, and What to Expect
Spironolactone was originally developed as a potassium-sparing diuretic for blood pressure and heart conditions, but its anti-androgenic properties have made it one of the most widely used systemic treatments for adult female hormonal acne. The mechanism operates through four pathways: competitive blockage of androgen receptors at the nuclear level, inhibition of androgen synthesis by blocking the enzyme responsible for converting androstenedione to testosterone, inhibition of 5-alpha reductase which reduces conversion of testosterone to its more potent form DHT, and an increase in sex hormone-binding globulin which reduces circulating free testosterone.
At the 2026 American Academy of Dermatology Annual Meeting in Denver, John S. Barbieri, MD, director of the Advanced Acne Therapeutics Clinic at Brigham and Women’s Hospital, presented data confirming that spironolactone performs as well as or better than oral antibiotics for women with acne, while eliminating the antibiotic resistance risk associated with long-term antibiotic use. The 2026 AAD report confirming spironolactone as a first-line systemic treatment for women with acne based on updated clinical trial data aligns with what Perfect B has seen in practice.
The ideal candidate for spironolactone at Perfect B is an adult woman with deep cystic acne concentrated in the lower face, confirmed androgen elevation or sensitivity on labs, and a history of inadequate response to topical treatments alone. It is not appropriate for use during pregnancy due to its anti-androgenic effects, and patients with certain electrolyte or kidney concerns require closer monitoring. Standard dosing for acne ranges from 50 to 200 mg daily, typically started at lower doses and adjusted based on response and tolerability.
Why Living in Miami Makes Hormonal Acne Harder to Manage
Miami adds a whole extra layer to hormonal acne that most clinical protocols written for general audiences do not account for. Humidity, constant sweating, reapplying sunscreen over skin that has not been properly cleaned first, late nights, alcohol, and the chronic low-grade cortisol elevation that comes with a high-stimulation environment. It is a perfect storm for hormonal chaos. Patients in South Florida are dealing with conditions that compound the internal hormonal load with external triggers that keep inflammation running higher than it would in a drier, lower-stress climate.
At Perfect B in Doral, the protocol accounts for this reality specifically. Product recommendations include non-comedogenic formulations that hold up in high humidity without trapping sweat and sebum against the skin. Cleansing timing matters more here than in most climates: patients who wear sunscreen through a Miami afternoon need to cleanse before reapplying, not just layer on top. Cortisol management is addressed as a clinical component rather than a lifestyle suggestion, because the data from the lab panel often shows elevated cortisol in patients whose breakout patterns track closely with work stress, social schedules, and sleep disruption. Our clinical guide to microneedling in Miami covers how SkinPen combined with exosomes and PDRN addresses both active acne damage and the post-inflammatory texture that Miami patients consistently deal with after breakout cycles.
What Our Patients Experience in the First 90 Days
Patients who have been battling hormonal acne for years often arrive at Perfect B with a specific kind of exhaustion. They have tried the products, read the articles, followed the routines, and gotten inconsistent results at best. The frustration is not from lack of effort. It is from applying the right effort to the wrong problem. You cannot scrub hormonal acne away. The inside has to be fixed first, and then the outside gets cleaned up.
In the first four weeks, the focus is on getting the labs back, reviewing the full hormonal picture, initiating the appropriate lane of the protocol, and adjusting the skincare routine to support rather than fight the treatment. Weeks four through eight is when the pattern starts to shift. New deep cysts stop forming as consistently. Existing lesions resolve without new ones appearing in the same location the following week. By week eight to twelve, the deep cysts stop forming. The skin calms down. It is not flawless yet at month three, but it is quiet. And for most patients who have been battling angry breakouts for years, that silence is everything.
Month three is when the work shifts to what comes next. Once the hormonal component is quiet, the focus moves to scarring, post-inflammatory hyperpigmentation, and the texture damage left behind by years of deep cysts. That is where the real transformation happens. Chemical peels, microneedling, and targeted in-office procedures address the visible record of the breakout history while the hormonal protocol keeps new lesions from forming. Patience and commitment are the non-negotiable ingredients throughout.
Hormonal Acne After 40: Perimenopause, PCOS, and What Changes in the Protocol
One of the most consistent surprises for patients over 40 is discovering that hormonal acne is not just a teenage problem. Perimenopause hormonal acne is more common than most providers acknowledge, and it often presents in women who had clear skin throughout their twenties and thirties. As estrogen levels decline in perimenopause, the relative androgenic activity on the skin increases even if absolute testosterone levels have not risen. The sebaceous glands respond to this shift by producing more sebum, the skin’s inflammatory response becomes less regulated, and the same deep cyst pattern that defines younger hormonal acne appears in a patient who was never prone to breakouts before.
The protocol for perimenopausal hormonal acne is not identical to the protocol for a 28-year-old with androgen excess. The lab picture is different, the hormonal trajectory is different, and the co-occurring skin changes mean that the treatment approach has to be calibrated accordingly. Retinoids remain effective but require a gentler introduction. Spironolactone is still appropriate for the right candidate but often needs closer monitoring in the context of other perimenopausal medications. PCOS is the other major driver of hormonal acne in adult women that requires its own clinical attention. At Perfect B, patients presenting with acne alongside irregular cycles, unexplained weight changes, or excess hair growth are evaluated for PCOS specifically before the acne treatment protocol is finalized. Our clinical perspective on hormonal imbalance covers how cortisol, insulin, estrogen decline, and metabolic changes interact and how Perfect B builds protocols that address the full hormonal picture in women navigating perimenopause.

Frequently Asked Questions
1. What is hormonal acne and how is it different from regular acne?
Hormonal acne is adult-onset acne driven by fluctuations in androgens, primarily testosterone and DHEA-S, which increase sebum production and trigger deep inflammation in the skin. Unlike adolescent acne which tends to appear across the forehead and nose, hormonal acne in adults concentrates along the jawline, chin, and lower cheeks. It presents as deep, painful cysts rather than surface-level blackheads, and it follows a cyclical pattern tied to the menstrual cycle, stress levels, or hormonal conditions like PCOS.
2. What labs should be tested before treating hormonal acne?
At Perfect B, we run free and total testosterone, DHEA-S, cortisol, fasting insulin, and vitamin D before building any hormonal acne protocol. DHEA-S is an adrenal androgen that many providers overlook, and low vitamin D levels appear consistently in patients with persistent inflammatory acne. These markers tell us where the imbalance is coming from before we decide how to treat it.
3. Does spironolactone work for hormonal acne?
Spironolactone is one of the most effective systemic treatments available for adult women with hormonal acne. It works by blocking androgen receptors in the skin and reducing sebum production through multiple pathways. Clinical data from the 2026 American Academy of Dermatology Annual Meeting confirmed its role as a first-line treatment for women with acne, with effectiveness comparable to or exceeding oral antibiotics without the long-term resistance risk.
4. How long does it take to cure hormonal acne?
There is no single timeline, but in our clinical experience at Perfect B most patients who want to know how to cure hormonal acne see the deep cysts stop forming within 90 days of a properly supervised protocol. The skin is not flawless at month three, but it is quiet. The full transformation from active breakouts to cleared and smooth skin typically takes six to nine months of consistent treatment.
5. Does hormonal acne go away on its own?
For most adult women it does not resolve without addressing the underlying hormonal driver. It can fluctuate with the menstrual cycle, improve temporarily, and return with the same pattern. Patients who wait frequently arrive at the clinic with not only active breakouts but accumulated scarring that requires additional treatment. The earlier the hormonal trigger is identified and addressed, the less collateral damage there is to repair.
6. Is hormonal acne worse in Miami?
Miami’s combination of heat, humidity, sweating, lifestyle stress, and chronic cortisol elevation creates specific challenges for hormonal acne. At Perfect B we adjust protocols for this reality with specific product recommendations, cleansing timing, and lifestyle guidance calibrated for South Florida patients.
7. What is the best treatment for hormonal acne in adults?
The best treatment is one built around your specific labs. At Perfect B we use a three-lane approach: custom topical regimens for mild cases, oral spironolactone for patients with deep jawline cysts, and in-office procedures including chemical peels and microneedling for scarring and pigmentation. Our clinical overview of acne scar types explains how scar type determines the treatment approach at Perfect B.
8. Can perimenopause cause hormonal acne?
Yes, and it is more common than most women expect. As estrogen levels decline in perimenopause, the relative effect of androgens on the skin increases, which can trigger acne for the first time in women who had clear skin through their twenties and thirties. The treatment approach for perimenopausal hormonal acne differs from younger women, and a proper lab workup is especially important before designing a protocol.
The Clinical Takeaway: Hormonal Acne Is an Inside Job
Every patient who has spent years trying to manage hormonal acne through topicals alone already knows that something is not adding up. The products change, the results stay the same. For anyone still searching for how to cure hormonal acne, the answer is consistent: start with the labs. The skin is where the symptom shows, but the driver is in the hormonal environment that the skin is responding to. The labs, the protocol, and the clinical oversight are what change that environment.
At Perfect B in Doral, FL, every hormonal acne patient gets the same starting point: labs first, protocol second. From there, the three-lane approach is built around what the data shows, whether that is a custom topical regimen, oral spironolactone, in-office procedures, or a combination across the treatment arc. We see patients from across Miami, Hialeah, Kendall, and Westchester who have been managing this condition on their own for years. The moment treatment addresses the internal driver rather than the external symptom, everything changes.
📍 Visit us at Perfect B, 3905 NW 107th Ave, Suite 104, Doral FL 33178
📞 Call or message us at (786) 502-2260


