

Perfect B, Doral Fl. | 05.11.26 | 8 min read.
This post is for educational purposes only and does not substitute for personalized medical advice. Treatment protocols vary by individual. Consult a licensed medical provider before beginning any treatment.
Most People Treating Fungal Acne Are Using the Wrong Treatment Entirely
If you have been treating what looks like acne for months with antibiotics, benzoyl peroxide, or retinoids and the breakout keeps coming back, there is a real possibility that you do not have bacterial acne at all. Pityrosporum folliculitis, also called malassezia folliculitis or fungal acne, is one of the most consistently misdiagnosed skin conditions in clinical practice. It looks like acne. It appears where acne appears. It frustrates patients the same way persistent acne does. But its cause is a yeast, not a bacterium, and every treatment that works for bacterial acne is useless against it.
At Perfect B in Doral, FL, we see this pattern regularly. A patient comes in after six months of oral doxycycline with a chest or forehead breakout that has not resolved, and in some cases has gotten worse. The antibiotic treatment shifted the bacterial flora on the skin, removed the competition, and gave the Malassezia yeast more room to grow. The treatment was actively feeding the problem.
Key Takeaways
- Pityrosporum folliculitis is caused by yeast, not bacteria, which means antibiotics, benzoyl peroxide, and most standard acne treatments have no effect and can actually worsen it by reducing bacterial competition.
- The most reliable distinguishing feature is itch: fungal acne causes significant itching, while regular acne vulgaris rarely itches at all.
- Fungal acne never produces comedones (blackheads or whiteheads) and the papules are strikingly uniform in size, unlike the mixed morphology of bacterial acne.
- Miami’s climate is one of the highest-risk environments in the continental US for pityrosporum folliculitis, with year-round heat, humidity above 70%, and conditions that favor Malassezia overgrowth consistently.
- Oral antifungals clear pityrosporum folliculitis rapidly, often within two to four weeks, but recurrence is common without maintenance and trigger management.
What Is Fungal Acne? (And Why the Name Is Technically Inaccurate)
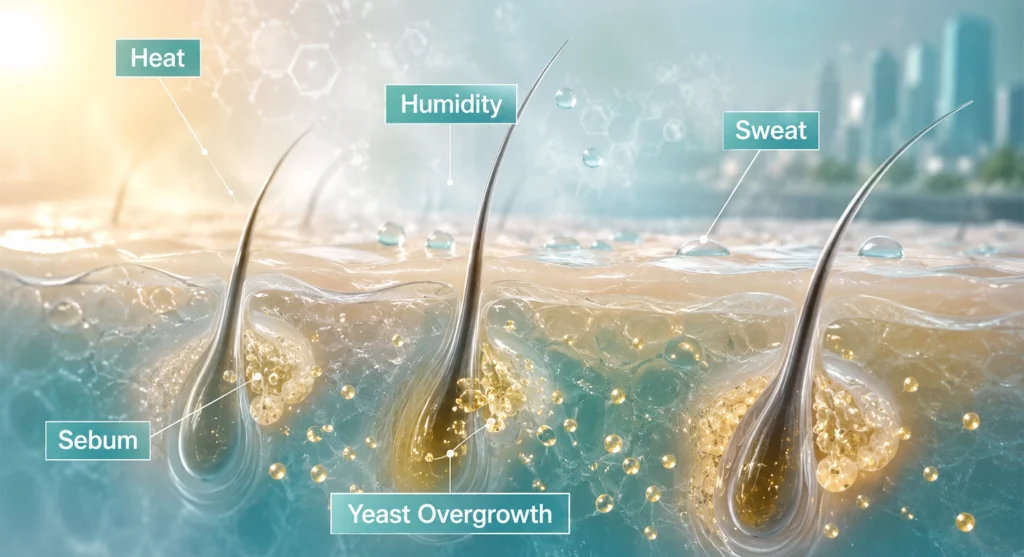
Fungal acne is a consumer term. The clinical diagnosis is pityrosporum folliculitis or malassezia folliculitis, named for the Malassezia yeast that causes it. Malassezia is a lipophilic yeast, meaning it feeds on the fatty acids in sebum, and it is a normal resident of healthy human skin. The condition develops not from an external infection but from an overgrowth of yeast that is already present, triggered by conditions that favor its proliferation.
Pityrosporum folliculitis and malassezia folliculitis: the same condition, two names
The condition has gone by both names in the clinical literature. Pityrosporum was the historical genus name for the yeast; the current classification uses Malassezia. Both terms refer to the same infection of the pilosebaceous unit, specifically the hair follicle and its associated sebaceous gland, by overgrown Malassezia yeast species, particularly M. globosa, M. sympodialis, and M. restricta. A peer-reviewed article in the Journal of Clinical and Aesthetic Dermatology documenting that Malassezia folliculitis is a fungal acneiform condition commonly misdiagnosed as acne vulgaris that often persists for years without resolution when treated with standard acne antibiotics encapsulates exactly what we observe in clinical practice.
Why Malassezia lives on your skin but does not always cause problems
The yeast exists on the skin of most adults without causing visible symptoms. Folliculitis develops when specific conditions shift the balance: antibiotic use that eliminates competing bacteria, heat and humidity that increase sebum production and sweat, occlusion from tight or synthetic clothing, oily skincare products that feed the yeast, or immune suppression from medications or illness. Remove those conditions and the yeast returns to a harmless level. Leave them in place and the follicular infection persists regardless of whatever antibacterial treatment is applied. → Learn how Perfect B’s acne treatment plan in Doral, FL distinguishes between fungal and bacterial causes before designing a protocol, ensuring the treatment actually matches the diagnosis.
Fungal Acne vs Regular Acne: The 5 Clinical Differences That Matter
The distinction between pityrosporum folliculitis and acne vulgaris is visible to a trained eye, but it is consistently missed in general practice because patients and many providers focus on what the breakout looks like at a glance rather than its specific characteristics. Here are the five clinical markers that separate them.

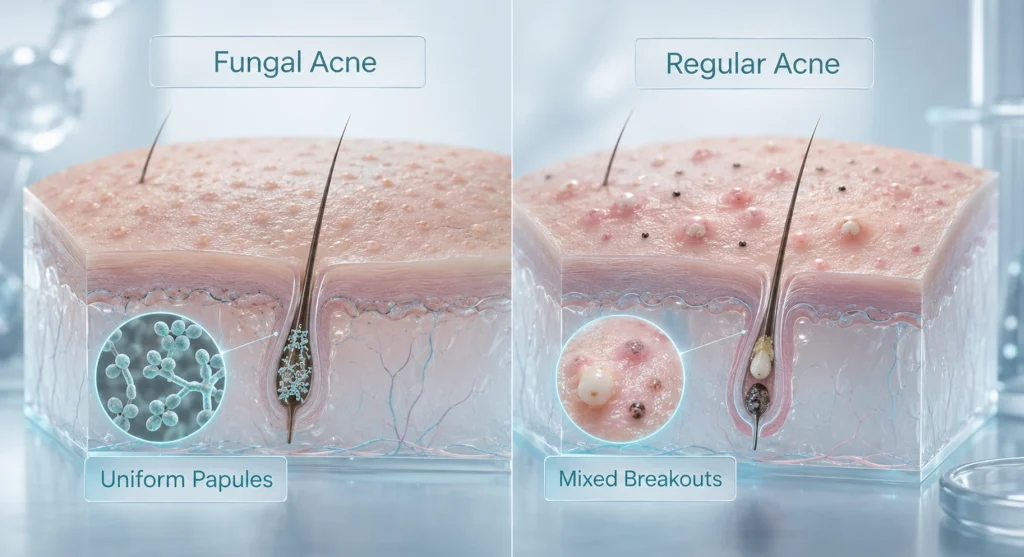
1. Appearance: uniform vs mixed morphology
Pityrosporum folliculitis produces papules and pustules that are strikingly uniform in size, typically 1 to 2 millimeters, clustered in the same areas, all at roughly the same stage of development. When you look at a patch of fungal acne, it looks consistent. Acne vulgaris produces a mixed picture: different sizes, different types (papules, pustules, nodules, cysts), different stages of development in the same zone. The monomorphic pattern of fungal acne is one of its most reliable visual markers.
2. Itch: the symptom that changes the diagnosis
Fungal acne itches, often intensely. Regular acne almost never itches. This is the single fastest clinical question to ask a patient: if the breakout is itchy, pityrosporum folliculitis moves immediately to the top of the differential. Most patients who have been treating their breakout as bacterial acne report that they noticed itching but assumed it was from the products they were using, not the condition itself. It is not.
3. Location patterns: chest, back, forehead vs facial acne zones
Pityrosporum folliculitis most commonly appears on the upper back, chest, shoulders, and forehead, particularly along the hairline. These are the areas with the highest density of sebaceous follicles and the most occlusion from clothing and hair. Acne vulgaris follows the sebaceous gland distribution of the face: T-zone, cheeks, jaw, chin. Both conditions can appear on the face, which is part of what makes the diagnosis complicated, but the pattern is different. Fungal acne on the forehead tends to appear as a band or cluster along the hairline rather than distributed across the face.
4. Response to treatment: the clearest diagnostic clue
If a breakout has been treated with antibiotics or standard acne medications for more than eight weeks without meaningful improvement, pityrosporum folliculitis should be suspected. In many cases, antibiotic treatment makes fungal acne worse by reducing the bacterial population that normally competes with Malassezia yeast. Patients on long courses of doxycycline, minocycline, or tetracycline who develop or worsen a chest or back breakout during treatment are a classic clinical presentation. The treatment is not failing because the acne is resistant. The treatment is failing because the diagnosis is wrong.
5. Comedones: the one thing fungal acne never has
Comedones, both open (blackheads) and closed (whiteheads), are a defining feature of acne vulgaris. They form when sebum and dead skin cells plug a follicular opening. Pityrosporum folliculitis does not produce comedones. If a breakout includes blackheads or whiteheads, at least part of the condition is acne vulgaris. A breakout with no comedones at all is far more suspicious for fungal origin.
What Causes Pityrosporum Folliculitis? The Miami Climate Factor
Pityrosporum folliculitis is not randomly distributed. It clusters in hot, humid climates, among people who sweat heavily, and in patients who have recently taken antibiotics. South Florida checks all of those boxes year-round, which is why we see this condition more frequently at Perfect B in Doral than a clinic in a drier, cooler region would.
Heat and humidity as primary triggers in South Florida
Miami’s average humidity stays above 70% for most of the year. The combination of heat and moisture creates persistently elevated sebum production, increased sweating, and a skin environment that Malassezia thrives in. Patients who exercise outdoors, spend extended time in air-conditioning that alternates with outdoor heat, or wear athletic or synthetic fabrics that trap moisture against the skin are at significantly higher risk. At Perfect B, we see clear seasonal patterns: flares peak in late summer when humidity and heat are at their maximum, but in Miami the risk window is essentially year-round. The chart below shows the correlation between Miami’s monthly humidity levels and estimated Malassezia flare risk.
Antibiotics: how treating bacterial acne can make fungal acne worse
Oral antibiotics eliminate the bacterial competition on the skin surface that normally keeps Malassezia in check. When that competition is removed, the yeast has more substrate and more territory. This is why patients who start doxycycline for acne sometimes notice a new type of breakout appearing on the chest or back during the first few months of treatment: they have shifted their skin ecology in a direction that favors fungal overgrowth. This does not mean antibiotics are always the wrong choice for acne, but it does mean that any new or worsening truncal breakout during antibiotic therapy should trigger clinical consideration of pityrosporum folliculitis.
Other triggers: oily products, sweating, immunosuppression
Malassezia feeds on C11 to C24 fatty acids found in many skincare oils, particularly coconut oil, olive oil, and many emollient moisturizers. Heavy, oil-based products applied to the chest, back, or face create a feeding environment for the yeast. Patients using rich moisturizers or occlusive sunscreens in a hot climate are at higher risk. Immunosuppression from corticosteroids, HIV, or other conditions also significantly increases susceptibility. Adolescent males, who have higher sebum production and more pronounced hormonal fluctuations, are the demographic most commonly affected, but pityrosporum folliculitis affects adults of all ages and genders, particularly in high-humidity environments.
How Is Pityrosporum Folliculitis Diagnosed? What to Expect at Perfect B
The most common diagnostic pathway is clinical: a provider evaluates the appearance, distribution, and symptom pattern of the breakout and uses the distinguishing features described above to differentiate it from acne vulgaris. In many cases, the clinical picture is clear enough that laboratory confirmation is not necessary. When the diagnosis is uncertain, a KOH (potassium hydroxide) preparation from a follicular scraping can demonstrate the yeast under microscopy, and a Wood’s lamp examination may show yellow-green fluorescence in affected areas.
Why Fitzpatrick III-V patients get misdiagnosed more often in Miami
In patients with Fitzpatrick III to V skin tones, which describes the majority of our patient population in Doral given the heavily Latin American and Caribbean demographics of South Florida, the erythema (redness) around follicular papules is less visually pronounced. The uniform papules of pityrosporum folliculitis can be harder to distinguish from acne at a glance in melanin-rich skin, and the itch symptom is more likely to be attributed to other causes. This increases the risk of prolonged misdiagnosis and prolonged antibiotic treatment that worsens the underlying condition. At Perfect B, we specifically screen for pityrosporum folliculitis in any patient with a truncal breakout that has not responded to standard acne treatment, regardless of skin tone.
When you should suspect fungal acne over regular acne
Suspect pityrosporum folliculitis when: the breakout is itchy; the papules are uniform in size; there are no comedones; the breakout is located primarily on the chest, back, or forehead hairline; standard acne treatments have not worked after two to three months; or antibiotic treatment is in progress and a new truncal breakout has appeared. Any one of these features warrants clinical consideration. Multiple features together make the diagnosis highly probable before any laboratory confirmation is performed. → Read how Perfect B evaluates breakout patterns in adult patients to determine whether hormonal changes, bacterial acne, or fungal folliculitis is driving the condition, and how each requires a different treatment approach.
Can You Have Both Fungal Acne and Regular Acne at the Same Time?
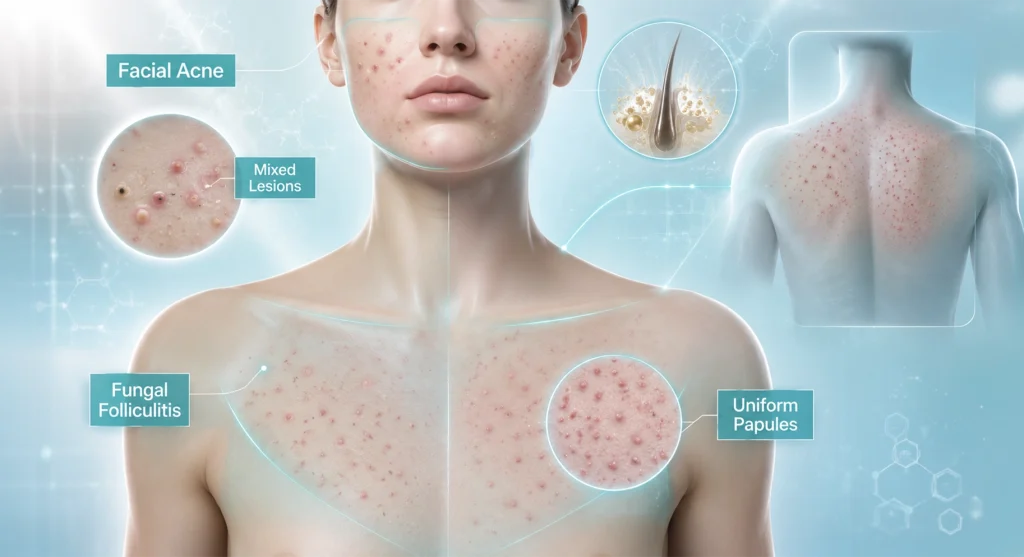
Yes, and this is more common than most patients realize. Pityrosporum folliculitis and acne vulgaris can coexist, and this coexistence is part of what makes the condition so difficult to manage without a proper clinical evaluation. A patient may have genuine bacterial acne on the face alongside malassezia folliculitis on the chest and back. Treating only the bacterial component leaves the fungal component untreated and vice versa.
What coexisting conditions look like clinically
In patients with both conditions simultaneously, the facial acne often shows the mixed morphology typical of acne vulgaris, including comedones, while the truncal breakout shows the uniform, itch-associated papules of pityrosporum folliculitis. The clinical approach at Perfect B in this scenario is to address both concurrently: antifungal treatment for the folliculitis and an appropriate acne protocol for the facial component. Treating only one without the other produces partial improvement that leads patients to conclude treatment is not working, when in reality the wrong component is being treated.
How to Treat Pityrosporum Folliculitis: Topical vs Oral Antifungals
Because pityrosporum folliculitis is a fungal infection, the only effective treatments are antifungal agents. The choice between topical and oral treatment depends on the severity and extent of the condition.
First-line topical treatment: ketoconazole and selenium sulfide
For mild cases or as maintenance therapy, topical antifungals are effective. Ketoconazole 2% shampoo or cream, applied to affected areas and left for several minutes before rinsing, is the most commonly used topical agent. Selenium sulfide 2.5% shampoo works similarly. Both can be used as a body wash on affected areas two to three times per week. In clinical practice, topical treatment alone is often insufficient for active pityrosporum folliculitis because the yeast is located deep within the follicle, below the surface penetration depth of most topical agents. Topical treatment is most effective for maintenance after the initial infection has been cleared with oral antifungals.
When oral antifungals are needed and what to expect
Oral antifungals are the most effective treatment for active pityrosporum folliculitis. Fluconazole and itraconazole are the most commonly prescribed. A clinical study in Dermatology Reports documenting treatment outcomes for Malassezia folliculitis confirming that oral itraconazole at 100 mg achieves rapid improvement, with most patients clearing in two to four weeks when compared to topical ketoconazole alone reflects the consistent clinical experience we see in practice. Most patients notice significant improvement within two to three weeks of starting oral treatment. The yeast is located deep in the follicle, and oral agents reach it systemically in a way topical products cannot. Recurrence after stopping treatment is common, which is why maintenance topical protocols are recommended even after clearance.
Why benzoyl peroxide and antibiotics do not work
Benzoyl peroxide kills bacteria by oxidation. It has no antifungal mechanism. Antibiotics eliminate bacteria by disrupting cell wall synthesis or protein production. Yeast have a fundamentally different cellular structure and are unaffected by these mechanisms. Using either on pityrosporum folliculitis produces no direct effect on the yeast and, in the case of antibiotics, removes the bacterial competition that normally keeps Malassezia populations in check. This is not a nuanced or controversial point: it is a basic microbiological principle that these treatments simply cannot work against a yeast infection.
Skincare Ingredients to Avoid During Treatment and What to Use Instead
Malassezia feeds on C11 to C24 fatty acids, which means specific skincare ingredients actively worsen the condition during treatment. Avoiding these is as important as using the antifungal treatment itself.
Avoid during treatment: coconut oil, olive oil, argan oil, squalane derived from olive sources, fatty acid-rich moisturizers, sunscreens with high oleic acid content, and any product with lauric, myristic, palmitic, or stearic acids high in the ingredient list. These all provide substrate for Malassezia growth.
Use instead: mineral sunscreens with non-comedogenic bases, fragrance-free gel or water-based moisturizers, niacinamide serums (which have some antifungal properties), and zinc pyrithione-containing cleansers, which inhibit Malassezia without the full antifungal potency of ketoconazole but provide a useful adjunct. → See how Perfect B approaches the selection of adjunct skincare treatments alongside clinical procedures for acne-related conditions, including which ingredients and protocols are appropriate when fungal activity is a concern.

Will Pityrosporum Folliculitis Come Back? Managing Recurrence in a Humid Climate
Recurrence after successful treatment is the rule, not the exception, particularly in South Florida’s climate. Malassezia is a permanent resident of the skin. The treatment clears the overgrowth and the follicular infection, but the yeast remains present. Any return of the triggering conditions, whether heat, sweating, antibiotics, or oily products, can restart the cycle.
Effective recurrence management includes: using an antifungal shampoo as a body wash once or twice per week on affected areas as ongoing maintenance, avoiding oil-based products on chest and back year-round, managing sweat exposure with post-exercise showering and moisture-wicking fabrics, and communicating pityrosporum folliculitis history to any provider who recommends antibiotic treatment for any condition. In Miami’s climate, maintenance is not optional for patients who have had pityrosporum folliculitis. Without it, the condition reliably returns. → For patients who developed scarring from prolonged or recurrent breakouts before a correct diagnosis was made, Perfect B’s microneedling for acne scars protocol addresses post-inflammatory changes regardless of the original breakout cause.
Frequently Asked Questions
1. How do I know if I have pityrosporum folliculitis or regular acne?
The fastest clinical questions are: does the breakout itch (fungal acne does, regular acne rarely does), are the bumps uniform in size (fungal acne yes, regular acne no), and are there any blackheads or whiteheads (regular acne yes, fungal acne never). If the breakout itches, is on the chest or back, has uniform small papules, and has not responded to standard acne treatments, pityrosporum folliculitis is the most likely diagnosis. A clinical evaluation at a medical aesthetics provider or dermatologist can confirm it, sometimes with a KOH test.
2. Can pityrosporum folliculitis clear on its own without treatment?
In some cases, if the triggering factor is removed, the condition can improve. A patient who develops pityrosporum folliculitis during antibiotic therapy may see improvement after stopping the antibiotic. But in most cases, particularly in a high-humidity climate like Miami, the condition does not fully resolve without antifungal treatment. The yeast overgrowth within the follicle requires antifungal intervention to clear, and leaving it untreated risks scarring and prolonged discomfort.
3. How long does treatment take to work?
Most patients see significant improvement within two to four weeks of starting oral antifungal treatment. The papules flatten and the itch resolves before the skin fully clears. Complete clearance typically takes four to six weeks with oral treatment. Topical-only treatment takes longer and may not fully clear deep follicular involvement. Maintenance therapy should begin immediately after clearance to prevent recurrence.
4. Is fungal acne contagious?
No. Pityrosporum folliculitis develops from an overgrowth of yeast that is already present on the patient’s own skin. It is not transmitted between people. Malassezia is a normal skin commensal that every adult carries. The condition arises from the internal conditions that allow it to overgrow, not from contact with an infected person.
5. Can I use tretinoin or other retinoids if I have pityrosporum folliculitis?
Retinoids do not directly treat or worsen pityrosporum folliculitis, but if the folliculitis is the primary diagnosis, retinoids will have no meaningful effect on it. If a patient has both acne vulgaris and pityrosporum folliculitis simultaneously, retinoids may address the bacterial component while antifungals address the yeast component. The treatment should match the actual diagnosis in each zone of breakout.
6. Does diet affect pityrosporum folliculitis?
The evidence for dietary influence on pityrosporum folliculitis specifically is limited compared to dietary research on acne vulgaris. However, because Malassezia feeds on fatty acids, diets very high in certain fats may theoretically influence sebum composition in a way that affects yeast growth. More practically, high-glycemic diets increase sebum production generally, which provides more substrate for Malassezia. There is no established dietary protocol for pityrosporum folliculitis the way there is for hormonal acne, but patients with recurrent cases who eat high-glycemic diets may benefit from addressing that component alongside antifungal maintenance. Contact us at (786) 502-2260 to discuss a comprehensive treatment approach for your specific presentation.
Closing: Getting the Diagnosis Right Is the Entire Treatment
Pityrosporum folliculitis is not a rare or exotic condition. It affects a meaningful percentage of patients who present with what appears to be treatment-resistant acne, and in Miami’s climate it is a more frequent clinical finding than in most other US markets. The condition is entirely treatable. The problem is not the treatment itself, it is the frequency with which the wrong treatment is applied for months before the correct diagnosis is made. Every month of antibiotic therapy applied to a yeast infection is a month of ineffective treatment, unnecessary antibiotic exposure, and continued skin damage from an unresolved infection.
The most important clinical step is asking the right questions before prescribing. Does it itch? Are the papules uniform? Are there no comedones? Has standard acne treatment failed? If the answers point toward pityrosporum folliculitis, the treatment path is clear and the results are rapid. At Perfect B in Doral, we build the evaluation of fungal vs bacterial acne into every new patient consultation specifically because the Miami environment makes this diagnosis more common and more likely to be missed before patients reach us. → Schedule a consultation at Perfect B in Doral, FL to have your breakout pattern properly evaluated and receive a treatment protocol that matches the actual cause, whether bacterial, fungal, hormonal, or a combination.
📍 Visit us at Perfect B, Doral FL
📞 Call or message us at (786) 502-2260


