

Perfect B, Doral Fl. | 06.01.26 | 9 min read.
This content is for educational purposes only and does not substitute for medical advice. Peptide therapy must be prescribed and supervised by a licensed medical provider. Do not begin a peptide protocol without a clinical evaluation. For medically guided care, see how peptide therapy is delivered under medical supervision at our Doral clinic as part of a complete, individualized plan.
Skip Ahead to the Perfect B Peptide Protocol Tool. See Reconstitution, Daily Units, and Cycle Structure.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
What You Need Before Your First Peptide Injection
Before drawing a single dose, patients need the correct equipment. Using the wrong syringe or needle is one of the most common sources of injection pain and inaccurate dosing. The materials list is short, but each item matters.
Syringe and Needle Selection: Gauge, Length, and Why It Matters
For subcutaneous peptide injection, the standard setup is a U-100 insulin syringe with a 27 to 29 gauge needle and a half-inch (12.7mm) shaft. The gauge number refers to needle thickness: the higher the gauge, the thinner the needle. A 29 gauge needle produces significantly less discomfort than a 25 gauge needle and is thin enough that most patients describe the sensation as a mild pinch rather than a sting.
A half-inch needle length is appropriate for most subcutaneous injection sites in adults. Patients with very low body fat may use a 5/16-inch needle; patients with more adipose tissue at the injection site do not need a longer needle, since subcutaneous tissue is typically reached within the first few millimeters of insertion.
- 29 gauge, 1/2 inch: the standard for most peptide protocols, including BPC-157, CJC-1295/Ipamorelin, and GHK-Cu
- 27 gauge, 1/2 inch: acceptable alternative, slightly wider bore makes drawing viscous solutions easier
- U-100, 1mL capacity: the correct syringe volume for most peptide doses, with clear graduations for accurate measurement
Bacteriostatic Water vs Sterile Water: Why the Distinction Matters
Lyophilized peptides (the powdered form dispensed by compounding pharmacies) require reconstitution before injection. Bacteriostatic water, which contains 0.9% benzyl alcohol as a preservative, is the correct choice for multi-dose vials because it prevents bacterial growth between uses. Sterile water, which contains no preservative, is appropriate only for single-use vials. Using sterile water in a multi-dose vial creates a contamination risk once the stopper is punctured. Your prescribing provider or compounding pharmacy will confirm which to use based on your specific protocol.
Key Takeaways
- Needle standard: a 27 to 29 gauge, half-inch insulin syringe is the correct tool for subcutaneous peptide injection in most adults.
- Best injection sites: the abdominal wall (two inches from the navel) and the outer thigh are the two most reliable sites for self-administration.
- Site rotation: rotating across a mapped grid prevents scar tissue accumulation and maintains consistent absorption over multi-month cycles.
- Frequency varies by peptide: BPC-157 is typically dosed twice daily; CJC-1295/Ipamorelin is dosed once nightly; MOTS-c and GHK-Cu follow their own schedules based on mechanism.
- Nodules are expected with BPC-157: small subcutaneous bumps at the injection site are a normal depot response, not infection, and resolve within two to three days without intervention.

The Best Subcutaneous Injection Sites for Peptides
Subcutaneous tissue, the layer of fat just beneath the skin, is the target for peptide injection. Not all sites on the body provide equal access to this layer or equal comfort during injection. The three primary sites used in clinical peptide protocols are the abdominal wall, the outer thigh, and the upper arm, with the abdomen being the preferred starting point for most patients.
The Abdominal Wall: Why Most Protocols Start Here
The abdominal wall provides the most accessible and consistent subcutaneous layer on the body. The target zone is a band running roughly two inches on either side of the navel, staying at least two inches away from the navel itself. This area has enough adipose tissue in most adults to make subcutaneous needle placement straightforward, and it is easy to observe and pinch during self-injection. The abdomen also tends to have less nerve density than the thigh at the specific insertion points used, which translates to less sensation during injection.
The Thigh: The Best Alternative for Active Patients
The outer portion of the upper thigh, midway between the knee and the hip, is the second most commonly used site. Patients who are very lean in the abdominal area or who experience more discomfort there often find the thigh more comfortable. Athletes and patients with active training schedules should avoid injecting into the thigh on heavy leg training days, as increased blood flow to active muscle can alter peptide absorption timing.
Site Rotation: How to Track It and Why It Matters
Injecting repeatedly into the same spot causes lipodystrophy, a breakdown of subcutaneous fat that creates permanent indentations and can impair peptide absorption at that site. The standard approach is to divide each injection zone into a grid of smaller areas and rotate through them systematically, never returning to the same spot within two to three days. A simple tracking method is to use a small notebook or phone calendar entry after each injection, noting the site and side used. Patients on twice-daily protocols, such as BPC-157, benefit especially from a mapped rotation system across both the abdomen and thigh.
How to Inject Peptides Subcutaneously: The 8-Step Protocol
The steps below apply to the standard subcutaneous injection technique used for most clinical peptide protocols. Each step exists for a specific reason, and skipping any one of them introduces contamination risk or dosing error.
Step 1: Wash Hands and Prepare the Workspace
Wash hands thoroughly with soap and water for at least 20 seconds. Work on a clean, flat surface. Remove the peptide vial from the refrigerator and allow it to reach room temperature for five to ten minutes, as cold solutions tend to cause more discomfort on injection.
Step 2: Clean the Vial Stopper
Wipe the rubber stopper of the peptide vial with a fresh alcohol swab using a single, firm stroke. Allow it to air dry for ten seconds. Do not blow on it or wave it dry; moving air introduces contaminants.
Step 3: Draw the Correct Dose
Pull back the syringe plunger to draw air equal to your prescribed dose volume. Insert the needle into the vial stopper, inject the air (this equalizes pressure and makes drawing easier), then invert the vial and draw the peptide solution to the correct graduation mark on the syringe. Tap the syringe lightly to move any air bubbles upward, then push them out with a small press of the plunger.
Step 4: Select and Clean the Injection Site
Choose the next site in your rotation. Wipe the area with a fresh alcohol swab using a single stroke outward from the center. Allow it to dry completely before injecting. Injecting through wet alcohol causes stinging and can carry trace alcohol into the subcutaneous layer.
Step 5: Pinch the Skin When Needed
For patients with less subcutaneous fat at the injection site, pinching a small fold of skin between the thumb and forefinger raises the subcutaneous layer away from the muscle beneath. This is most relevant at the thigh and abdomen in lean patients. Patients with adequate adipose tissue at the site do not need to pinch.
Step 6: Insert the Needle at the Correct Angle
For a half-inch needle, insert at 45 degrees to the skin surface when using the pinch technique or when injecting at a lean site. Insert at 90 degrees (straight in) when there is sufficient tissue depth and no pinch is needed. The needle should enter smoothly. If resistance is felt immediately, the angle is off; withdraw and reposition. The full half-inch length should be inserted for consistent subcutaneous placement.
Step 7: Inject Slowly and Withdraw
Press the plunger slowly and steadily over two to three seconds. Rapid injection is one of the primary causes of nodule formation and post-injection discomfort. Once the plunger is fully depressed, withdraw the needle at the same angle it was inserted. Apply light pressure to the site with a clean gauze pad for a few seconds, without rubbing.
Step 8: Dispose and Log the Injection
Dispose of the used syringe immediately in a sharps container. Do not recap the needle. Note the injection site in your log and refrigerate the vial. Single-use syringes must never be reused; reusing needles causes barb formation on the tip, which significantly increases injection pain and tissue damage.
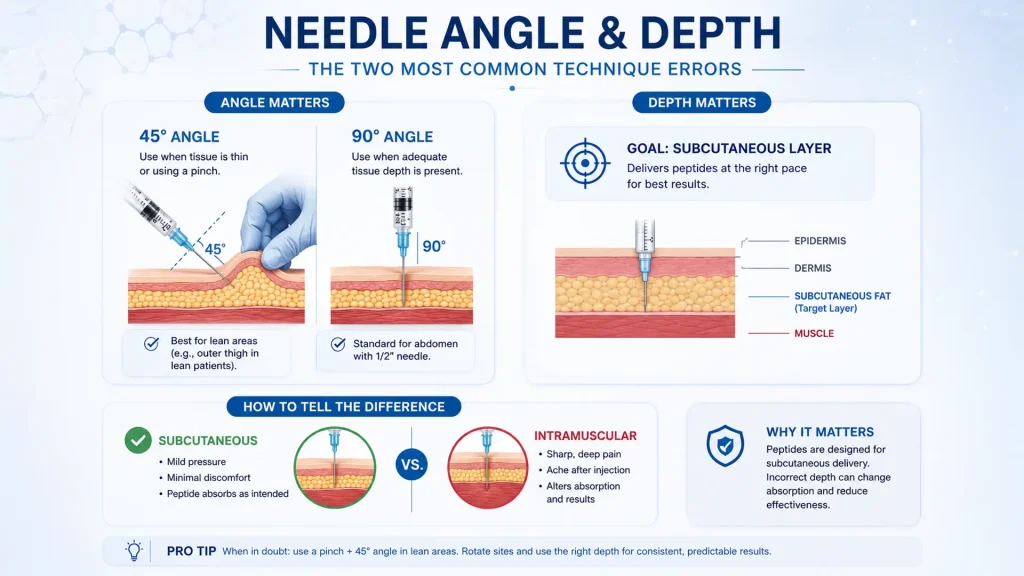
Needle Angle and Depth: The Two Most Common Technique Errors
Of all the variables in peptide injection technique, needle angle and insertion depth generate the most patient questions and the most preventable complications.
45 Degrees vs 90 Degrees: Choosing the Right Angle
The 45-degree angle is appropriate when the subcutaneous fat layer is thin, specifically when the pinch technique is used or when injecting at a site with limited adipose tissue. The 90-degree angle (straight in) is appropriate when adequate tissue depth is present and no pinch is needed. Using a 90-degree angle without sufficient tissue depth risks injecting into muscle. For most adults using a half-inch needle at the abdomen, 90 degrees is standard. For the outer thigh in lean patients, 45 degrees with a pinch is the safer choice.
How to Recognize an Intramuscular vs Subcutaneous Injection
An intramuscular injection at a subcutaneous site produces sharper, deeper pain on insertion and a more pronounced ache after withdrawal. Subcutaneous injection typically produces only mild surface-level pressure. Peptides designed for subcutaneous delivery, which includes most clinically prescribed options such as BPC-157, CJC-1295/Ipamorelin, and GHK-Cu, are formulated for subcutaneous absorption rates. According to a 2017 systematic review in the Journal of Clinical Nursing confirming that aspiration before subcutaneous injection does not reduce adverse events, subcutaneous injections carry a distinct pharmacokinetic profile that intramuscular delivery disrupts, which is why correct angle and depth matter for predictable results.
How Often Should You Inject Peptides? Frequency by Protocol
Injection frequency is not universal. It is determined by the pharmacokinetics of each specific peptide, the therapeutic goal, and the cycle structure prescribed. The most common error patients make is applying one peptide’s frequency to another. The schedules below reflect standard clinical practice for the protocols prescribed at Perfect B.
BPC-157 and TB-500: Frequency and Timing
BPC-157 is typically administered twice daily, morning and evening, to maintain consistent tissue-level concentrations throughout the day. Our complete BPC-157 dosage protocol covers the full cycle structure, loading phase options, and how to time injections around training and meals for patients using this peptide for injury recovery or gut health at Perfect B in Doral, FL. TB-500 is dosed less frequently, typically once or twice per week during a loading phase and once every two weeks during maintenance, reflecting its longer half-life and systemic distribution pattern.
CJC-1295/Ipamorelin and MOTS-c: The Timing Logic
CJC-1295/Ipamorelin is administered once nightly, typically 30 to 60 minutes before sleep. This timing is deliberate: the combination amplifies the natural growth hormone pulse that occurs during slow-wave sleep, making evening dosing significantly more effective than morning dosing for body composition and recovery goals. MOTS-c is typically administered in the morning to align with metabolic activity cycles. Its mechanism targets cellular energy production, and morning dosing allows the peptide to act during the body’s peak metabolic period.
GHK-Cu and Epithalon: Different Schedules for Different Goals
GHK-Cu is typically administered once daily as part of skin or hair restoration protocols. Epithalon is administered in defined cycles of ten to twenty days with rest periods between them, responding to pulse-dosing rather than continuous daily administration due to its mechanism of telomere regulation and circadian rhythm modulation.
Lumps and Nodules at the Injection Site: What They Mean
BPC-157 Nodules: Why They Form and What to Do
BPC-157 has a well-documented tendency to form small subcutaneous depot nodules at the injection site. These are pea-sized or smaller, mildly firm to the touch, and typically painless. They represent a local concentration of the peptide solution in the subcutaneous layer rather than rapid dispersion. The cause is almost always injection speed: depressing the plunger too quickly does not allow the solution time to distribute. Slowing the injection to three to five seconds is usually sufficient to eliminate nodule formation. Nodules that do form from BPC-157 resolve without treatment within two to three days. Our clinical review of peptide therapy safety explains the broader range of injection site responses patients may experience and which ones require clinical evaluation versus simple observation.
When to Contact Your Provider
Contact your prescribing provider if a nodule is warm to the touch, red, expanding rather than shrinking over 48 hours, or accompanied by fever. These signs may indicate infection at the injection site, which requires evaluation and treatment. Patients using medical-grade compounded peptides from a licensed pharmacy rather than unregulated online sources have significantly lower rates of injection site reactions. The FDA’s guidance on compounding pharmacies outlines the legal and quality differences between licensed compounded medications and research compounds sold without a prescription, which directly affects injection site safety.
What Peptide Injection Training Looks Like at Perfect B in Doral
At our clinic in Doral, FL, no patient leaves with a peptide kit before completing an in-office injection training session with one of our providers. The session covers equipment setup, dose calculation from the reconstitution chart, site selection for the specific protocol, and a supervised practice injection so patients can feel the correct technique before doing it alone at home. The most common errors we see from patients who learned via YouTube or unvetted online guides are incorrect needle angle (too steep for their body composition), alcohol not fully dried before injecting, and plunger depression too fast for BPC-157. All three are correctable in two minutes during a supervised session and take weeks to self-correct through trial and error.
Our peptide therapy program at Perfect B in Doral, FL includes the clinical evaluation, protocol design, compounded peptide kit, reconstitution supplies, and an in-office training session before patients administer their first dose at home. Patients in the Miami area who are already on a protocol prescribed elsewhere and need hands-on injection guidance can schedule a single technique consultation.

Frequently Asked Questions
1. What gauge needle is best for peptide injection?
A 27 to 29 gauge needle is the clinical standard for subcutaneous peptide injection. The higher the gauge number, the thinner the needle and the less discomfort on insertion. Most patients find 29 gauge to be nearly pain-free at properly prepared sites. Needles below 25 gauge are too wide for comfortable subcutaneous self-injection.
2. Can you inject peptides into the thigh?
Yes. The outer thigh, midway between the hip and the knee, is a reliable subcutaneous injection site and is the preferred alternative when the abdomen is uncomfortable or if site rotation requires a break from abdominal injections. Avoid injecting into the thigh on heavy leg training days, as increased local blood flow may alter absorption timing.
3. How often should you inject peptides?
Frequency depends on the specific peptide. BPC-157 is typically dosed twice daily. CJC-1295/Ipamorelin is dosed once nightly. TB-500 is typically once or twice per week during loading. GHK-Cu follows a daily or every-other-day schedule. MOTS-c is generally dosed once daily in the morning. Your prescribing provider determines the schedule based on your specific therapeutic goal and cycle structure.
4. What angle should you inject peptides at?
Use a 45-degree angle with a skin pinch when subcutaneous fat at the site is limited. Use a 90-degree angle when there is adequate tissue depth and no pinch is needed. For most adults injecting into the abdominal wall with a half-inch needle, 90 degrees is appropriate. At the thigh in lean patients, 45 degrees with a pinch is safer to avoid muscle penetration.
5. Why do I have a lump after injecting BPC-157?
Small subcutaneous nodules after BPC-157 injection are a common and benign response. They form when the injection is administered too quickly and the solution pools rather than dispersing. Slowing the injection to three to five seconds eliminates the problem in most cases. Nodules from BPC-157 resolve without treatment within two to three days. If the nodule is warm, expanding, or accompanied by redness or fever, contact your provider.
6. Do you need to aspirate before injecting peptides subcutaneously?
No. Aspiration is not required for subcutaneous injections. Current clinical guidelines no longer recommend aspiration for subcutaneous sites because major blood vessels are not located in the subcutaneous layer. Aspiration is relevant for specific intramuscular injection sites, not for subcutaneous peptide administration.
Not Sure Which Peptide Protocol Fits Your Goals? See What Perfect B Patients With Similar Goals Are Running.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
Closing: The Technique Is Part of the Protocol
Peptide therapy outcomes depend on two equal pillars: the quality of the peptide and the consistency of the administration. A clinically prescribed BPC-157 protocol from a compounding pharmacy produces diminished results if the injection is too fast, too deep, or always at the same spot. The technique described in this guide takes under three minutes per injection once learned, and the learning curve is short for most patients. The ones who see the most consistent results are the ones who treat the injection protocol as part of the treatment, not an afterthought to it.
South Florida patients who want supervised injection training or a full peptide protocol evaluation can contact Perfect B directly.
- 📍 Visit us at Perfect B, Doral FL, serving Miami and South Florida patients seeking clinical peptide therapy.
- 📞 Call or message us at (786) 502-2260 to schedule your peptide injection consultation with a licensed medical provider.


