

Perfect B, Doral FL. | 03.21.25 | 8 min read.
This content is for educational purposes only and does not constitute medical advice. Consult a qualified medical provider before beginning any peptide therapy.
Perfect B does not offer Sermorelin. We prescribe NAD+ therapy and CJC-1295/Ipamorelin for the goals discussed in this comparison. This article explains how NAD+ and Sermorelin differ at the mechanism level for patients researching both options. Our prescription practice for growth hormone optimization is CJC-1295/Ipamorelin, not Sermorelin, and the clinical reasoning is explained in the closing section.
NAD+ vs Sermorelin: Two Therapies, Two Completely Different Mechanisms
When patients come in asking about peptide therapy for energy, recovery, and aging, the conversation frequently lands on two options: NAD+ and Sermorelin. At Perfect B we offer NAD+ therapy. We do not offer Sermorelin; our growth hormone protocol is CJC-1295/Ipamorelin, which is described in the closing section. Both NAD+ and Sermorelin produce real, measurable results when administered through a supervised clinical protocol, but they target different physiological systems. But they do not do the same thing, and prescribing one when the other is indicated is one of the most common mistakes in the peptide space.
NAD+ (nicotinamide adenine dinucleotide) is a coenzyme found in every cell of the body. It is essential for mitochondrial energy production, DNA repair, and neurotransmitter regulation. As we age, NAD+ levels decline significantly, which tracks with the fatigue, brain fog, and reduced cellular resilience that most patients describe. NAD+ therapy restores those depleted levels directly.
Sermorelin is a growth hormone-releasing hormone (GHRH) analog. It does not introduce exogenous HGH. Instead, it stimulates the pituitary gland to produce and release its own growth hormone in a pulsatile, physiologically normal pattern. This drives lean muscle production, fat metabolism, improved sleep quality, and tissue repair over weeks to months.
The distinction matters clinically. Choosing between them should not be arbitrary. It should follow the patient’s primary complaint, their labs, and their goals.
Key Takeaways
- NAD+ addresses cellular energy deficits: If fatigue, brain fog, and poor recovery are the primary complaints, NAD+ works faster and more directly on those mechanisms.
- Sermorelin addresses body composition and tissue quality: For patients losing muscle on a weight loss protocol or seeking long-term structural changes, Sermorelin is the more targeted choice.
- They work better together: Combined, NAD+ and Sermorelin target different systems simultaneously, which is why many patients eventually use both.
- Sleep alone warrants a different peptide: If poor sleep is the primary complaint with no other symptoms, Epithalon is often the first-line recommendation before either NAD+ or Sermorelin.
- Sermorelin is contraindicated in patients with a personal history of cancer due to its growth hormone-stimulating mechanism.
Who Should Start with NAD+ First?
The clearest indicator for starting with NAD+ is the patient who describes waking up tired despite sleeping a full night, experiencing mental sluggishness that does not resolve with caffeine, and feeling like their body takes longer to bounce back from physical exertion than it used to. These are the hallmarks of mitochondrial energy depletion, and NAD+ addresses that directly at the cellular level.
At Perfect B, when a patient presents with low energy, fatigue, and brain fog as their primary complaints, NAD+ is typically the first recommendation. It is excellent for restoring cellular energy and helping patients feel more rested and alert. The results are relatively fast compared to peptide therapies like Sermorelin, with most patients reporting a noticeable shift in energy and focus within two to four weeks of beginning NAD+ therapy.
NAD+ is particularly well-suited for patients in their 40s and 50s who are experiencing cognitive changes alongside physical fatigue. Research consistently links age-related NAD+ decline to both neurological performance and metabolic function. For these patients, restoring NAD+ levels is often described as recalibrating the baseline from which everything else improves.

Who Should Start with Sermorelin First?
Sermorelin becomes the priority when a patient’s goals or presentation shift toward body composition, muscle retention, and structural recovery. The clearest use case is a patient on an active weight loss protocol who is struggling to maintain or build lean muscle mass. GLP-1 medications like Tirzepatide and Semaglutide are highly effective for fat loss, but they do not preserve muscle. Patients losing weight rapidly without a supporting anabolic signal often find they are smaller but weaker, with less functional strength than before treatment.
At our clinic, the clearest clinical indicator for Sermorelin comes from patients on a weight loss protocol who are experiencing difficulty gaining or keeping muscle mass. “When a patient has been on a weight loss protocol and has been experiencing difficulty with gaining or keeping their muscle mass, I would recommend Sermorelin,” Valeria explains. Sermorelin addresses this by stimulating the body’s own growth hormone release, which supports lean muscle production, speeds tissue recovery, and improves the quality of deep sleep. In patients with difficulty gaining or keeping muscle mass, particularly those undergoing weight loss, Sermorelin is the more targeted intervention.
Sermorelin benefits also extend to the quality of aging broadly: skin texture, joint health, and bone density all respond to growth hormone over time. For patients focused on structural anti-aging rather than immediate energy, Sermorelin is typically the stronger long-term investment.
The timeline is longer than NAD+. Patients typically notice improved sleep onset within the first month. Measurable body composition changes, the kind visible in before and after comparisons, generally appear at eight to twelve weeks of consistent use.
What Happens When Patients Use Both NAD+ and Sermorelin Together?
The most common outcome when patients combine NAD+ and Sermorelin is that they achieve results neither therapy could produce alone. “They work great together because we can target the specific concern of increasing lean muscle while also improving overall energy and just feeling more focused and better overall with NAD+,” Valeria explains. The combination targets two distinct biological systems simultaneously. Sermorelin drives lean muscle production and structural body composition changes. NAD+ restores the cellular energy substrate that makes everything else work better: workouts feel more productive, recovery is faster, and cognitive clarity improves alongside the physical changes.
Patients in Miami and South Florida who are undergoing body recomposition protocols particularly benefit from this stack. The goal of recomposition, losing fat while building or maintaining muscle, requires both the anabolic signaling that Sermorelin provides and the mitochondrial efficiency that NAD+ restores.
In clinical practice, it is common to start with one therapy to address the most pressing complaint, assess the patient’s response, and add the second therapy in the following cycle. The combination is safe, well-tolerated, and synergistic. A useful framing from a clinical perspective: NAD+ helps patients feel better faster, while Sermorelin helps them function better overall. Together, they cover both dimensions.
For patients interested in a comprehensive NAD+ and peptide therapy program, our peptide treatment plan at Perfect B in Doral covers the full range of available therapies and how they are combined based on individual clinical goals.
Not sure which peptide protocol fits your goals?
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
When Would a Provider Recommend Epithalon Instead of NAD+ or Sermorelin?
This is one of the clinical nuances that tends to surprise patients who come in with a self-diagnosed need for either NAD+ or Sermorelin. When the primary complaint is poor sleep quality, specifically difficulty falling or staying asleep, and energy or muscle are secondary concerns, the first-line recommendation is often Epithalon rather than either of the more commonly discussed therapies.
Epithalon is a tetrapeptide that works through the pineal gland to regulate melatonin production and circadian rhythm. It has a well-documented effect on sleep architecture and has been studied for its anti-aging properties through telomere regulation. For a patient whose entire complaint can be summarized as “I cannot sleep and therefore everything else suffers,” addressing the sleep deficiency directly before layering in energy or anabolic therapies is the more precise clinical decision.
Once sleep quality is restored, reassessing for NAD+ or Sermorelin becomes much cleaner. Some patients find the other complaints resolve on their own once sleep is addressed.

Who Should Not Use Sermorelin?
The primary contraindication for Sermorelin is a personal history of cancer. Because Sermorelin works by stimulating growth hormone release, and growth hormone is a known driver of cell proliferation, any history of malignancy creates a meaningful risk. This applies even to cancers considered in remission. At our clinic, patients with any oncological history are screened carefully before any growth hormone-adjacent therapy is considered, and Sermorelin is routinely excluded from those protocols.
Other considerations include active thyroid dysfunction, pituitary disorders, or uncontrolled diabetes. Patients who are pregnant or nursing are also excluded. NAD+ does not carry the same growth-stimulating mechanism and is more broadly applicable across patient profiles, though dosing and delivery method still require clinical judgment.
How Long Does Each Therapy Take to Work? A Timeline Comparison
Timeline expectations are one of the most important things to calibrate before a patient begins either therapy. Misaligned expectations are the most common reason patients discontinue prematurely.
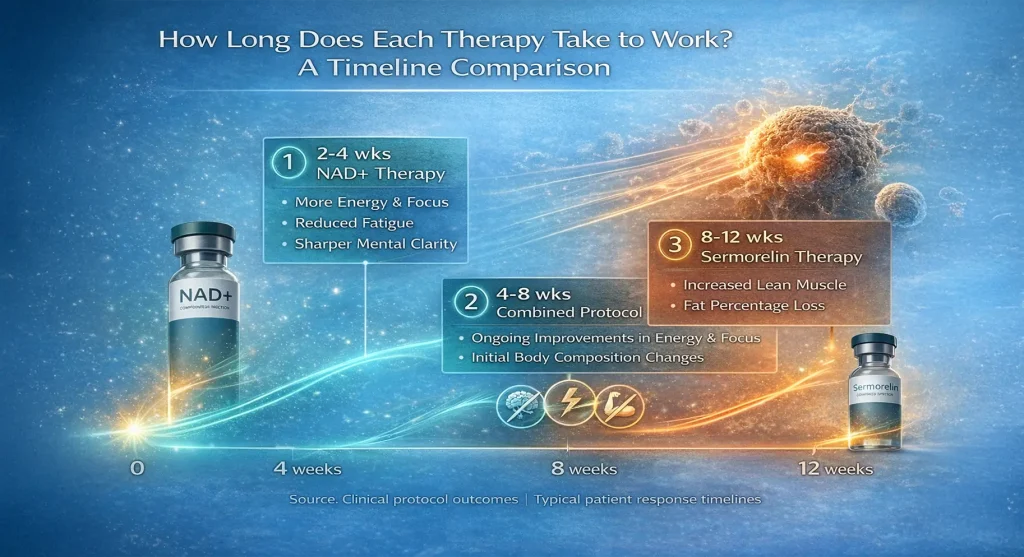
- NAD+ timeline: Most patients notice improved energy, reduced fatigue, and sharper mental clarity within two to four weeks of starting IV or injectable NAD+ therapy. The effect is relatively rapid because NAD+ replenishment works at the cellular level without requiring the body to upregulate a downstream hormonal cascade.
- Sermorelin sleep improvement: Improved sleep onset and sleep quality is typically the first effect patients notice, usually within the first month of consistent use.
- Sermorelin body composition changes: Measurable shifts in lean muscle mass and body fat percentage generally appear between eight and twelve weeks. This aligns with the natural cycle of growth hormone stimulation and the time required for meaningful tissue remodeling.
- Combined protocol: Patients using both therapies simultaneously tend to report subjective improvements in energy and focus first (from NAD+) followed by progressive body composition changes over months (from Sermorelin).
For a deeper look at how NAD+ therapy is used at our clinic and what to expect from a full treatment cycle, see our NAD+ treatment plan at Perfect B in Doral, FL.
NAD+ vs Sermorelin for Anti-Aging: What the Evidence Shows
Both therapies have meaningful anti-aging evidence, but they address different aspects of biological aging. A 2015 review in Cell Metabolism demonstrating that NAD+ precursor supplementation reverses mitochondrial dysfunction in aged muscle and restores metabolic function reinforced the mechanistic rationale for NAD+ as a longevity therapy. NAD+ decline is now understood as a driver of the mitochondrial dysfunction that underlies much of the physical and cognitive decline associated with aging.
Sermorelin’s anti-aging effects operate through the growth hormone axis. GH naturally declines beginning in the late 20s and accelerates after 40. This decline correlates with increases in visceral fat, decreases in lean mass, reduced bone density, and skin thinning. By restoring a more youthful GH secretion pattern without introducing exogenous hormone, Sermorelin targets these structural markers of aging. A review in the Journal of Clinical Endocrinology confirming that GHRH analog therapy produces significant improvements in body composition, sleep quality, and exercise capacity in aging adults supports its use in clinical anti-aging protocols.
For patients asking which one makes them “feel younger faster,” the clinical answer is NAD+ for the subjective experience of energy and clarity, and Sermorelin for the objective structural changes that show up in labs and the mirror over months.
See how NAD+ and Sermorelin fit into real patient protocols.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
Frequently Asked Questions
1. Can I use NAD+ and Sermorelin at the same time?
NAD+ and Sermorelin address different biological systems. Some clinics prescribe them together to target both cellular energy and growth hormone optimization simultaneously. At Perfect B we do not prescribe Sermorelin, so we do not run NAD+/Sermorelin combination protocols. For patients who want the same outcome the Sermorelin combination targets (energy plus structural body composition support), we combine NAD+ with CJC-1295/Ipamorelin, which produces stronger sustained GH pulses than Sermorelin’s brief single-pathway pulse.
2. How do I know if I need NAD+ or Sermorelin?
The decision typically comes down to your primary complaint. If you are waking up tired, struggling with brain fog, or feeling like your energy never fully returns after exertion, NAD+ is usually the first recommendation. If your primary concern is losing muscle during weight loss, difficulty building strength, or structural anti-aging goals, Sermorelin is typically the more targeted option. A clinical intake with labs helps confirm which system is most depleted.
3. How long before I feel results from Sermorelin?
Most patients notice improved sleep quality within the first month. Body composition changes, including increased lean muscle and reduced body fat, typically become measurable between eight and twelve weeks. Sermorelin requires consistent use over this timeframe because it works by gradually re-establishing a more youthful GH secretion pattern, not by introducing a sudden hormonal spike.
4. Is Sermorelin safe? Are there risks?
Sermorelin is generally well-tolerated when prescribed and monitored by a medical provider. The primary contraindication is a personal history of cancer, since its growth hormone-stimulating mechanism is not appropriate for patients with any oncological history. Other contraindications include uncontrolled thyroid disease, active pituitary disorders, and pregnancy. Side effects are typically mild and include injection site reactions or transient water retention.
5. What is Epithalon and when is it used instead of NAD+ or Sermorelin?
Epithalon is a tetrapeptide that works through the pineal gland to regulate melatonin and circadian rhythm. When poor sleep is a patient’s primary complaint and energy or muscle mass are secondary, Epithalon is often recommended first. Addressing the root sleep disruption directly can resolve downstream energy and recovery complaints without adding other therapies prematurely.
6. Does NAD+ therapy require IV administration?
NAD+ can be administered via IV infusion, intramuscular injection, or subcutaneous injection depending on the protocol and the patient. IV delivery is generally considered the most bioavailable method and is preferred for patients seeking faster systemic effect. At Perfect B, the delivery method is selected based on the patient’s goals, schedule, and clinical profile. Our NAD+ treatment plan at Perfect B in Doral covers the full range of delivery options available.
7. What is the difference between Sermorelin and Ipamorelin?
Both are growth hormone secretagogues, but they work through different receptors. Sermorelin mimics GHRH and acts on the pituitary directly. Ipamorelin works through the ghrelin receptor and has a more selective growth hormone pulse with fewer side effects related to cortisol and prolactin. They are often combined (CJC-1295 + Ipamorelin is a common stack) for a more complete GH stimulation pattern. Perfect B prescribes CJC-1295/Ipamorelin and does not prescribe Sermorelin. For patients comparing the two, the clinical reasoning is described in the closing section.
8. Does Perfect B offer Sermorelin in Doral, FL?
No. Perfect B prescribes CJC-1295/Ipamorelin for general growth hormone optimization and Tesamorelin for visceral fat reduction. We do not offer Sermorelin. This article compares NAD+ and Sermorelin because both are widely researched by patients pursuing peptide therapy, but Perfect B’s prescription practice is limited to NAD+, CJC-1295/Ipamorelin, Tesamorelin, and the other peptides listed in our peptide treatment plan. Patients on Sermorelin elsewhere considering switching can book a consultation for an evaluation.
Closing: The Clinical Bottom Line on NAD+ vs Sermorelin
NAD+ and Sermorelin are not interchangeable therapies chasing the same outcome. NAD+ is a fast-acting cellular repair and energy restoration tool. Sermorelin is a slower, structural intervention that reshapes body composition and supports long-term hormonal health. The right choice depends entirely on what is most depleted in the individual patient, and in many cases, both are appropriate once the primary complaint is addressed. Valeria Marulanda, our clinical lead, frames the comparison this way: “NAD+ restores cellular energy and helps patients feel better faster, and growth hormone peptides like CJC-1295/Ipamorelin support the structural anti-aging goals patients often associate with Sermorelin.” That framing holds across virtually every patient who presents asking which direction to take.
Perfect B does not prescribe Sermorelin. We prescribe NAD+ therapy and CJC-1295/Ipamorelin for the goals patients typically research Sermorelin for, because both produce stronger sustained clinical results in our patient population. Peptide therapy at Perfect B is always preceded by a clinical intake and discussion of goals. We do not recommend therapies based on trend or patient demand alone. The selection process is designed to match the treatment to the patient’s actual physiology, not to a generalized protocol. If you are in the Miami area and considering either therapy, a consultation is the right first step.
See what patients like you are running at Perfect B.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
- 📍 Visit us at Perfect B, 8200 NW 41st St, Doral FL 33166
- 📞 Call or message us today to schedule your peptide therapy consultation


