

Perfect B, Doral Fl. | 06.02.26 | 8 min read.
This content is for educational purposes only and is not a substitute for professional medical advice. Consult a licensed provider before beginning any scar treatment.
What Are Hypertrophic and Keloid Acne Scars?
Acne leaves two fundamentally different types of permanent scars, and they require opposite treatment strategies. Atrophic scars, including ice pick, boxcar, and rolling types, form when the skin loses tissue during healing, creating depressions below the surface. Hypertrophic and keloid scars form when the skin does the opposite: it overproduces collagen in response to the inflammatory insult of a deep acne lesion, creating a raised, firm mass of tissue above the surface.
According to DermNet, a peer-reviewed dermatology reference updated in 2026, hypertrophic scars are limited to the area of damaged skin while keloid scars grow beyond the original wound margin and are unlikely to regress on their own. In the context of acne, these raised scars occur most commonly on the jawline, chin, chest, and shoulders, particularly in patients with Fitzpatrick IV, V, and VI skin types who carry a higher genetic predisposition to exaggerated collagen responses.
For an overview of the full spectrum of acne scar types, see our complete guide to acne scar types and how Perfect B approaches each one. This post focuses specifically on the raised variants: what makes them difficult to treat, and what the clinical protocol actually involves.
Key Takeaways
- Raised acne scars form when the skin overproduces collagen during wound healing, creating firm elevated tissue above the skin surface rather than the depressions seen in atrophic scars.
- Hypertrophic scars stay within the original wound boundary and may partially improve over time. Keloid scars grow beyond the original wound, never resolve without treatment, and carry a significant recurrence risk after treatment.
- Intralesional corticosteroid injection is the evidence-based first-line treatment for both types. It suppresses fibroblast activity, reduces excess collagen, and flattens the scar over a series of sessions.
- A second phase addresses texture and color once the scar has been adequately flattened by steroid treatment. The sequence matters: laser or resurfacing before steroid flattening can worsen a raised scar.
- Keloid-prone patients in South Florida’s Hispanic and Latin American population require conservative protocols: lower starting doses, longer intervals, and careful monitoring to avoid triggering new keloid formation.
Hypertrophic vs. Keloid Scars: Why the Treatment Approach Is Different
The distinction between these two raised scar types is clinically significant because it directly affects treatment intensity, expected response, and recurrence risk.
Hypertrophic Acne Scars
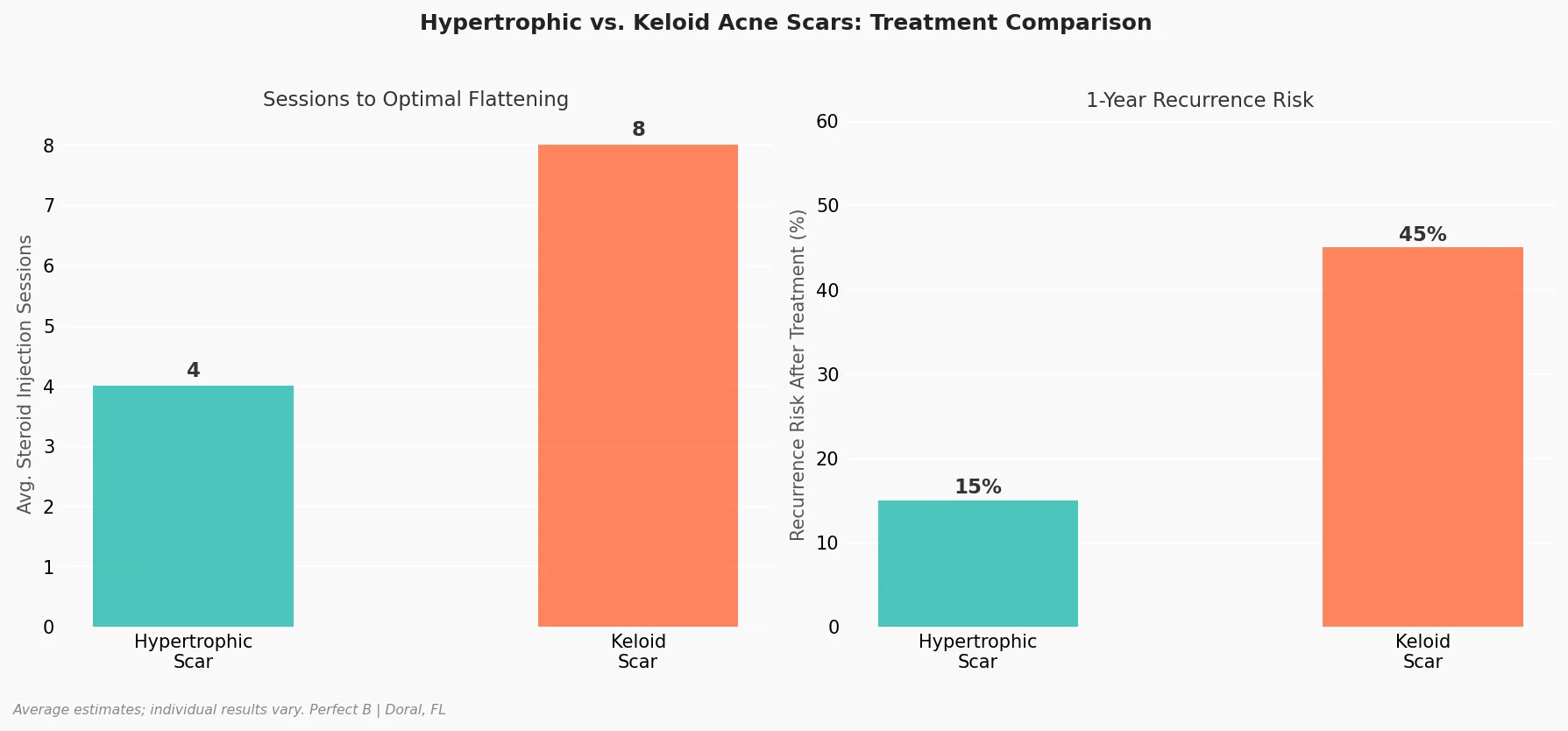
A hypertrophic scar is raised, firm, and typically pink to red. It stays within the exact boundaries of the original acne lesion. It develops 1 to 2 months after the pimple heals. Over years, it may become somewhat less noticeable on its own, though rarely disappears completely. Hypertrophic scars respond well to steroid injection treatment, with most patients seeing significant flattening within 3 to 5 sessions.
Keloid Acne Scars
A keloid scar grows beyond the original wound boundary. A pimple that was 5mm across may produce a keloid 1 to 2 cm in diameter. Keloids are red to purple, feel firm and sometimes tender or itchy, and develop months to years after the original acne lesion, not always immediately. They never resolve without intervention, carry a recurrence rate of up to 45% after treatment, and require a more conservative approach because aggressive treatment can trigger new keloid formation. Patients with keloid-prone skin on the face or chest from acne have often had previous treatments that worsened the scar.
The practical diagnostic distinction is the border: a hypertrophic scar matches the outline of the original pimple. A keloid is larger than the pimple ever was.
Why Raised Acne Scars Are Harder to Treat Than Pitted Scars

The treatments that work for pitted acne scars work by stimulating collagen production: microneedling, subcision, RF microneedling, PDRN. Applied to a raised scar, these same treatments would make the problem worse by adding more collagen to a zone where excess collagen is already the problem.
A 2023 peer-reviewed review of hypertrophic scarring in the journal Cells documents that hypertrophic scar tissue is characterized by aberrant wound healing with excessive extracellular matrix deposition and dysregulated fibroblast activity, the opposite of what drives atrophic scar formation. Treatment must suppress this activity, not stimulate it.
This is also why patients who have tried microneedling for raised acne scars and seen no improvement, or worsening, are not unusual. Microneedling is an excellent tool for atrophic scars. See our guide on microneedling for atrophic acne scars for the full explanation of when and why that approach is indicated.
Beyond the treatment mechanism, raised scars present the additional challenge of recurrence. Pitted scars that are treated do not return: the tissue that was lost has been rebuilt. Keloid scars have up to 45% recurrence within one year of treatment because the underlying genetic predisposition to overproduction remains. Management, not cure, is the accurate framing.
Steroid Injections for Raised Acne Scars: The First-Line Protocol
Intralesional corticosteroid injection (typically triamcinolone acetonide) is the established first-line clinical treatment for both hypertrophic and keloid acne scars. The corticosteroid is injected directly into the raised scar tissue using a fine needle. In the scar tissue, the corticosteroid suppresses fibroblast proliferation, reduces collagen and glycosaminoglycan synthesis, and breaks down the disorganized excess collagen that forms the raised bulk of the scar.
The result over a series of sessions is progressive flattening of the scar. The tissue softens, the height decreases, and the color typically shifts from red or purple toward the patient’s natural skin tone. The scar rarely reaches the level of completely normal surrounding skin, but significant reduction is achievable in most patients.
Protocol for Hypertrophic Acne Scars
Sessions are spaced 4 to 6 weeks apart to allow the steroid effect to manifest and avoid cumulative side effects such as skin atrophy or hypopigmentation. Most patients with hypertrophic acne scars on the face see meaningful improvement by session 3 and reach optimal flattening by session 4 to 6. Facial skin responds faster than body sites because of better vascular supply.
Protocol for Keloid Acne Scars
We use lower starting concentrations for keloid treatment than we would for hypertrophic scars, and we titrate upward based on response. The reason is biological: if the steroid dose is too high or causes significant local tissue reaction, it can trigger a new collagen response that enlarges the keloid rather than reducing it. Sessions are scheduled 6 to 8 weeks apart. Response is monitored carefully between sessions. The expected timeline is 6 to 10+ sessions before reaching the plateau of steroid response.
After Steroid Flattening: The Second Phase of Raised Scar Treatment
Once the scar has been adequately flattened by the steroid series, a second treatment phase can address what the steroid cannot: the surface texture, residual discoloration, and integration of the treated area with surrounding skin.
The sequence is non-negotiable. Laser resurfacing or any energy-based treatment applied to a still-raised scar creates a new wound healing event in tissue that is already prone to overproduction. This can trigger enlargement. We do not begin the second phase until the scar has reached its plateau response from steroids, typically confirmed across two consecutive sessions with no further measurable reduction.
The second phase at Perfect B uses resurfacing to smooth the surface of the treated area and blend it with the surrounding skin. Post-inflammatory hyperpigmentation often accompanies raised acne scars in Fitzpatrick IV-VI patients and requires its own concurrent management. See our guide on post-inflammatory hyperpigmentation for the full explanation of how dark marks from acne are treated alongside, but separately from, the structural scar.
What You Can Do Between Clinical Sessions: Silicone, Pressure, and SPF
Between steroid injection sessions, consistent at-home management extends the clinical effect and protects the treated tissue.
- Silicone gel or silicone sheets applied consistently for 12 or more hours daily create a moisture-rich, low-oxygen environment over the scar that reduces fibroblast activity and can soften hypertrophic scars between clinical sessions. Clinical evidence supports silicone as an effective adjunct to injection therapy, particularly for hypertrophic scars. Keloid response to silicone alone is more variable.
- SPF 30 or higher every morning over any actively treated scar is essential in South Florida. UV exposure to a scar under active treatment darkens post-inflammatory pigmentation, slows the collagen remodeling response, and counteracts what the steroid sessions are achieving. This is not optional.
- Avoid any trauma to the treated area between sessions. Picking at scabs, aggressive exfoliation, or new inflammatory acne in the same zone can trigger new keloid activity in susceptible patients. If active acne is still present, we address it first before beginning scar treatment.
How Many Sessions and What Results to Expect
The trajectory differs significantly between hypertrophic and keloid acne scars, and setting accurate expectations before treatment begins is part of the clinical standard of care at Perfect B.
Hypertrophic Acne Scars
- Sessions 1 to 2: Scar begins to soften. The firm texture becomes less hard to the touch. Color shifts from bright red toward pink.
- Sessions 3 to 4: Visible flattening. Scar height is measurably reduced. The treated area blends better with surrounding skin.
- Sessions 5 to 6: Optimal steroid response. Transition to second phase begins if texture improvement is needed.
- Second phase: Resurfacing smooths the surface. Most patients are satisfied by the end of the combined protocol.
Keloid Acne Scars
- Sessions 1 to 3: Conservative dosing phase. We assess response and monitor for signs of tolerance or adverse reaction before escalating dose.
- Sessions 4 to 8: Progressive flattening if the keloid is responding. Some keloids plateau early; this is expected, not failure.
- Plateau phase: The steroid series ends when two consecutive sessions show no further change. This is the stopping point, not the treatment failure point.
- Recurrence monitoring: We schedule follow-up at 3, 6, and 12 months. Keloids that begin regrowing are treated immediately, as early intervention is more effective than waiting for full recurrence.
What Patients at Our Doral Clinic See After Raised Scar Treatment
The patients who respond most consistently to raised acne scar treatment at Perfect B are those with hypertrophic scars from cystic acne on the jawline or chin, formed within the last 1 to 3 years, in patients who commit to the full initial series without stopping after the first visible improvement.
Our Doral patient population is predominantly Hispanic and Latin American, with a high proportion of Fitzpatrick IV and V skin types. This demographic carries a higher inherent keloid risk than average, and we see more raised scars here than clinics treating predominantly lighter skin tone populations. We calibrate every protocol accordingly: lower starting steroid concentrations, more cautious escalation, longer monitoring intervals. A patient in our practice does not receive the same protocol as a patient at a clinic that rarely treats keloid-prone skin.
Before and after results at our clinic for hypertrophic acne scars show consistent reduction in scar height and improved texture by the end of the steroid series, with further improvement through the resurfacing phase. Keloid results are more variable: some flatten dramatically, some plateau at 50 to 70% reduction. We discuss these realistic ranges at consultation because a patient who expects total elimination of a keloid will be disappointed, while a patient who understands meaningful reduction is achievable will be satisfied.
Who Is a Good Candidate and Who Needs a Different Approach First

Good Candidates
- Hypertrophic acne scars on the face that are 6 months to 3 years old and have not responded to topical treatments alone.
- Small to moderate keloid acne scars on the face or jawline, particularly in patients who have not previously received injections or whose prior treatment was suboptimal.
- Patients committed to multiple sessions over several months and realistic about partial improvement, especially for keloids.
- Patients with Fitzpatrick III-VI skin who understand the higher keloid risk and the conservative protocol it requires.
Who Needs a Different Approach First
- Patients with active, untreated acne producing new lesions in the same areas. We stabilize active breakouts before beginning scar treatment.
- Large or long-established keloids that have been present for decades and have reached significant size. These may require evaluation at a specialist facility that offers excision plus radiation therapy before injectable management.
- Patients who have had prior aggressive treatment (inappropriate laser or microneedling on a keloid) that enlarged the scar. These need a stabilization period and careful assessment before any new intervention.
Frequently Asked Questions
1. What is the difference between a hypertrophic scar and a keloid scar from acne?
Both form from excess collagen production during wound healing. The difference is location: a hypertrophic scar stays within the boundaries of the original pimple and may partially improve over time. A keloid grows beyond those boundaries, is larger than the original lesion, never resolves without treatment, and carries a high recurrence rate after treatment. Hypertrophic scars respond faster and more predictably to steroid injection than keloids.
2. Do keloid acne scars ever go away on their own?
No. Unlike hypertrophic scars, which may become less noticeable over years, keloid scars do not regress spontaneously. They require clinical intervention. Without treatment, they may continue to grow, especially in patients with active acne producing new inflammatory triggers in the same area.
3. How many steroid injections does it take to treat a raised acne scar?
Hypertrophic acne scars typically require 4 to 6 sessions spaced 4 to 6 weeks apart to reach optimal flattening. Keloid scars typically require 6 to 10 or more sessions, with a more conservative protocol and longer intervals between sessions. Response varies by scar age, location, size, and the patient’s genetic predisposition to excessive scarring.
4. Can keloid acne scars come back after treatment?
Yes. Keloids carry a recurrence risk of up to 45% within the first year after treatment. The recurrence risk is lower when the protocol is conservative, when silicone and SPF are used consistently between sessions, and when new inflammatory triggers (active acne) are controlled. Patients who develop early recurrence are treated immediately, which is more effective than waiting for full regrowth.
5. Is steroid injection treatment safe for darker skin tones?
Yes, with appropriate technique. The primary risk in Fitzpatrick IV-VI skin is hypopigmentation (lightening of the treated area) from over-injection or excessive steroid concentration. Using lower concentrations, controlled volumes, and consistent intervals between sessions significantly reduces this risk. Our protocols at Perfect B are specifically calibrated for the Fitzpatrick IV-V population that makes up the majority of our Doral patient base.
6. Will microneedling help my raised acne scars?
No microneedling is contraindicated for hypertrophic and keloid scars. Microneedling works by triggering a controlled wound healing response that stimulates collagen production. Applied to a scar where excess collagen is already the problem, this can worsen the raised scar. Microneedling is an effective treatment for atrophic (pitted) acne scars, which have the opposite problem. If you have raised scars, microneedling is not the right tool.
7. What is the difference between a raised acne scar and a dark spot from acne?
A raised acne scar (hypertrophic or keloid) has structural height above the surrounding skin surface it is a physical mass of excess collagen. A dark spot from acne, also called post-inflammatory hyperpigmentation, is a flat discoloration with no elevation. Dark spots are not scars and respond to different treatments. Many patients with raised scars also have PIH in the same areas, which we treat concurrently with a different approach.
8. What can I do at home between clinical sessions to help the treatment?
Silicone gel or sheets applied for 12 or more hours daily can complement injection treatment by reducing fibroblast activity between sessions, particularly for hypertrophic scars. SPF 30 or higher every morning protects the treated area from UV-induced pigmentation and slows collagen dysregulation. Avoiding any trauma, picking, or new acne in the treated zone is equally important, as new inflammation in keloid-prone skin can trigger recurrence during the treatment series.
The Clinical Bottom Line on Raised Acne Scar Treatment
Hypertrophic and keloid acne scars are not a cosmetic inconvenience that topicals can address. They are a structural excess of tissue produced by an overactive healing response, and they require clinical intervention that targets that mechanism directly. The two-phase protocol, corticosteroid injection to suppress and flatten followed by resurfacing to refine, addresses raised acne scars as the biological problem they are.
For patients in Doral and across South Florida, where the demographic profile carries a higher keloid risk than the national average, conservative and correctly sequenced treatment is not just a preference. It is a clinical necessity. The question is not whether raised acne scars can be improved. Most of them can. The question is whether the protocol is calibrated correctly for your skin type and your scar.
The next step is a consultation. Call or text Perfect B at (786) 502-2260 or see the full acne treatment plan at the link below.
- 📍 Visit us at Perfect B, Doral FL, serving Miami and South Florida patients seeking acne scar treatment.
- 📞 Call or message us at (786) 502-2260 to schedule your raised acne scar consultation with a licensed medical provider.
→ See Perfect B’s full acne treatment plan in Doral, FL and what to expect at your first consultation.


