

Perfect B, Doral Fl. | 06.03.26 | 9 min read.
This content is for educational purposes only and is not a substitute for professional medical advice. PDRN injection is a medical procedure that requires evaluation and supervision by a licensed provider. Patients should not attempt self-injection.
Why Stretch Marks Are Harder to Treat Than Other Scars
Stretch marks are not a surface skin problem. They are scars that form inside the reticular dermis when collagen and elastin fibers rupture under rapid mechanical stretching, during pregnancy, adolescent growth spurts, rapid weight change, or muscle gain. The damage happens from the inside out, which is why topical treatments applied to the skin surface have limited clinical evidence behind them. Collagen and elastin are not accessible to a product sitting on the epidermis.
The challenge that makes stretch marks harder to treat than other types of scars is structural. When the dermis tears, it does not heal with normal tissue architecture. The collagen that replaces the ruptured fibers is disorganized, the elastin network is disrupted, and the skin in the affected zone has permanently different mechanical properties than the tissue around it. That is why stretch marks do not simply fade completely over time in the way a surface bruise or superficial wound does. The structural change in the dermis is the target that treatment has to address.
At our clinic in Doral, we treat stretch marks on the abdomen, glutes, legs, and arms with a combination protocol that addresses exactly this structural deficit. The modalities we use, including RF microneedling with Morpheus8, microneedling with SkinPen, the ResurFx non-ablative fractional laser, and PDRN as a regenerative biologic, are each targeting the same underlying problem from different mechanisms. Our stretch mark reduction treatment plan at Perfect B covers all of these modalities, what each one does, and how they are sequenced depending on the stage and severity of the striae being treated.
Key Takeaways
- PDRN is a clinical injection, not a topical product. The PDRN serums sold on Amazon and at Korean beauty retailers are cosmetic products applied to intact skin. Medical-grade PDRN injected into the dermis delivers concentrated polynucleotide chains directly to the tissue that needs repair.
- Striae rubrae (red, new stretch marks) respond better to PDRN than striae albae (white, mature ones) because active vascularity and inflammation give the treatment more to work with. Timing matters more for this treatment than for almost any other stretch mark intervention.
- PDRN activates the A2A adenosine receptor in dermal fibroblasts, triggering production of collagen, elastin, and endogenous hyaluronic acid while also reducing local inflammation. This is a different mechanism than laser or RF microneedling, which is why combination protocols outperform single-modality approaches.
- Clinical studies show 80 to 90 percent of patients see meaningful improvement in stretch mark severity after a series of PDRN sessions, with measurable changes in volume, roughness, and skin smoothness documented at 20 weeks.
- South Florida patients with Fitzpatrick III-VI skin tones require adjusted session spacing to manage post-inflammatory hyperpigmentation risk when combining PDRN with microneedling or laser. This is especially relevant in Miami, where year-round UV exposure is a clinical consideration throughout the treatment period.
What PDRN Is and Why Scarred Dermal Tissue Responds to It
PDRN stands for polydeoxyribonucleotide. It is a purified extract derived from the DNA of salmon sperm cells, specifically chains of 50 to 2,000 deoxyribonucleotide base pairs. Despite its unconventional origin, the molecular structure is relevant because human cells recognize and process these fragments through specific receptor pathways that trigger tissue repair responses.
The primary mechanism is activation of the adenosine A2A receptor on dermal fibroblasts. When PDRN binds to this receptor, it initiates a cascade that increases cyclic AMP and activates protein kinase A, which in turn stimulates the fibroblasts to produce collagen, elastin, and endogenous hyaluronic acid. PDRN also promotes angiogenesis by increasing vascular endothelial growth factor (VEGF) expression, which improves microcirculation in the treated tissue, and it exerts a direct anti-inflammatory effect by suppressing pro-inflammatory cytokine pathways.
Stretch mark tissue is a particularly good target for PDRN because the problem is precisely what PDRN addresses. The disorganized collagen and disrupted elastin network in striae represent a structural deficit in fibroblast output. PDRN does not just stimulate general wound healing; it specifically promotes the production of the extracellular matrix components that are missing or disordered in scarred dermal tissue. In addition, PDRN fragments are used by cells in what is called the salvage pathway, a process by which cells recycle available nucleotides into new DNA synthesis rather than building new nucleotides from scratch. This supports cellular proliferation in the tissue around the striae, which contributes to the visible improvement in skin quality around and within the treated area.

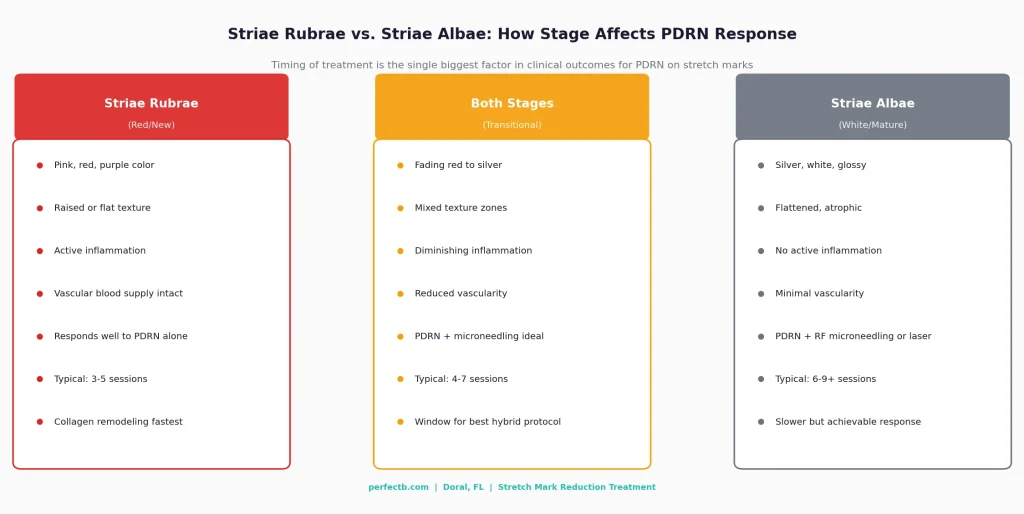
Striae Rubrae vs. Striae Albae: Why the Stage Changes the Protocol
The clinical vocabulary for stretch marks distinguishes two stages that behave very differently under treatment. Striae rubrae are the fresh, active phase: pink, red, purple, or dark brown marks that still have blood supply and local inflammatory activity. Striae albae are the mature phase: the marks have lost their vascularity, turned silvery or white, and the tissue has settled into its final atrophic state.
This distinction matters more for PDRN than for almost any other stretch mark modality because PDRN works partly through the vascular mechanism. When PDRN is injected into striae rubrae, it can interact with active fibroblasts in tissue that still has blood supply and an ongoing, if disorganized, repair process. The A2A receptor activation adds regenerative signal to tissue that is already metabolically active. When striae are still red, early intervention with PDRN can significantly influence the quality of the collagen matrix that forms as the marks mature. Treatment during this window consistently produces better outcomes than waiting for marks to fully mature.
Striae albae are not non-responsive to PDRN, but the mechanism shifts. Without active vascularity, the treatment relies more on the mechanical delivery of PDRN through microneedling channels and the direct stimulation of fibroblasts that are present but quiescent. In practice, mature white stretch marks require a combination approach to achieve meaningful improvement. At Perfect B, this typically means PDRN paired with either SkinPen microneedling or Morpheus8 RF microneedling, depending on the depth and density of the striae being treated.
What the Clinical Evidence Shows for PDRN on Stretch Marks
A 2024 review of polynucleotides in aesthetic medicine published in the International Journal of Molecular Sciences examined current clinical evidence across applications including stretch marks, confirming that PDRN activates the A2A adenosine receptor pathway to stimulate collagen synthesis, improve skin elasticity, and reduce inflammatory markers in treated dermal tissue. The review placed the mechanism within a broader body of evidence on PDRN for scar and atrophic tissue, noting that the salvage pathway contribution supports cellular proliferation beyond the direct receptor activation effect.
The clinical outcome data for PDRN specifically in stretch marks includes a 20-week randomized study in which polynucleotide injections produced significant reductions in stretch mark volume, roughness, and width, with improvements in Manchester Scar Scale scores documented at the end of the study period. Separately, a clinical series reported that 80 percent of patients saw remarkable scar reduction following three PDRN sessions, and a 2022 study found that 90 percent of patients experienced visible and lasting improvements in skin texture after completing a full series of polynucleotide injections. An independent study documented that 85 percent of patients showed notable reduction in stretch mark severity, with improvement across volume, width, and skin smoothness measures, and the treatment was well tolerated with minimal adverse effects across skin types.
Research published on the A2A receptor mechanism in PDRN tissue repair confirmed that PDRN treatment significantly increases migration of damaged cells and promotes new vessel formation through A2A receptor signaling, with the regenerative effect blocked when the A2A receptor is specifically antagonized, establishing the mechanism as the primary driver of the clinical outcomes observed. This mechanistic confirmation is relevant for understanding why PDRN works differently on striae rubrae versus albae: receptor density and local vascularity both affect how effectively the A2A pathway can be engaged.
A more recent investigation compared PDRN alone, fractional CO2 laser alone, and the combination of both for striae distensae in a randomized intraindividual clinical trial. The combination protocol produced the strongest results, while the laser-only arm carried elevated risk of post-inflammatory hyperpigmentation, particularly for patients with darker skin tones. This finding directly informs how we structure treatment at Perfect B for Fitzpatrick III-VI patients, where we sequence PDRN with microneedling and laser at adjusted parameters rather than leading with aggressive laser as the primary modality.
How PDRN Is Administered for Stretch Marks at a Medical Clinic
The PDRN serums marketed to consumers are applied topically to intact skin and cannot reach the reticular dermis. The clinical application that the study evidence supports requires delivering PDRN into the dermis directly, through one of two methods: mesotherapy injection or microneedling-assisted delivery.
Mesotherapy Injection
In the mesotherapy approach, PDRN is administered via a series of small, superficial injections placed directly into the dermis along the stretch mark zone. This is the same delivery method used in our PDRN protocols for other applications, including the under-eye area and neck lines. The provider uses a fine-gauge needle to place the solution in the dermal layer at regular intervals across the treatment area. Sessions are typically 30 to 45 minutes depending on the surface area being treated. The abdomen or thigh, the most common areas for stretch marks at our clinic, can cover a larger zone than the under-eye or neck, so session time reflects the treatment field.
Microneedling-Assisted Delivery
The second delivery method pairs PDRN with our SkinPen microneedling treatment. The mechanical action of the pen creates controlled micro-channels in the dermis while PDRN is applied topically during the procedure. The microchannels allow PDRN to penetrate below the stratum corneum, reaching dermal fibroblasts that a topical application on intact skin would never access. The microneedling also independently stimulates collagen induction by triggering the skin repair response through the controlled injury, and PDRN amplifies that response biochemically by providing the A2A receptor signal on top of the mechanical stimulus. We use this combined approach specifically for patients with a broader surface area of striae albae, where the mechanical induction from microneedling adds to what PDRN can accomplish through the receptor pathway alone.
PDRN Alone vs. PDRN With Microneedling: When the Combination Makes Clinical Sense
Whether PDRN works best on its own or in combination depends primarily on the stage of the stretch marks and the skin tone of the patient.
- PDRN alone via mesotherapy is most appropriate for striae rubrae, where the active inflammation and vascularity mean the A2A receptor pathway has good conditions to work in. For early-stage red marks, particularly on patients with Fitzpatrick III-VI skin who need to minimize additional procedural trauma to manage PIH risk, starting with PDRN mesotherapy sessions before introducing microneedling or laser can produce strong outcomes without adding thermal or mechanical stress to already-reactive tissue.
- PDRN combined with SkinPen microneedling is the standard protocol for striae albae with moderate coverage. The mechanical induction from microneedling creates the repair signal in atrophic tissue that has lost its ability to respond on its own. PDRN then amplifies the fibroblast response triggered by that signal. The combination consistently outperforms either treatment alone for mature white stretch marks.
- PDRN combined with Morpheus8 RF microneedling is appropriate for deeper or denser striae where the radiofrequency energy can address the deeper layers of the dermis that standard microneedling does not reach. Morpheus8 delivers RF energy at adjustable depths up to 7mm, which allows treatment of the reticular dermis where the most significant collagen disruption occurs in severe stretch marks. PDRN is incorporated into the protocol to enhance the regenerative response in the tissue.
- PDRN combined with ResurFx fractional non-ablative laser is used when surface texture improvement is a specific goal alongside dermal remodeling. The ResurFx StellarM22 1565nm fractional targets the superficial dermis and epidermis to improve the appearance of the skin overlying the striae while PDRN works at the deeper dermal level.
The decision about which combination to use is made at the consultation based on the patient profile, not from a standard menu. Stretch mark stage, surface area, skin tone, history of prior treatments, and the specific zones being treated all influence the plan.
What to Expect: Sessions, Results, and Timeline
Stretch mark treatment requires multiple sessions because the dermal remodeling process does not complete in a single appointment. The general clinical framework at Perfect B for stretch mark reduction runs from 3 to 9 months, with sessions scheduled every 2 to 6 weeks depending on the specific modalities being used and how the skin is responding.
- Sessions 1-3: Initial PDRN or PDRN with microneedling. The first three sessions establish the baseline regenerative response. Some patients notice improvement in skin texture and hydration around the striae within two to four weeks of the first session, though changes in the marks themselves tend to become more visible after the second or third treatment.
- Sessions 4-6: Protocol adjustments based on response. For striae rubrae that are responding well to PDRN mesotherapy, sessions may continue without modification. For striae albae or areas not responding as expected, this is when the protocol may shift to include Morpheus8 or ResurFx to address deeper or surface-level factors.
- Sessions 7-9+: Maintenance and completion. The final sessions focus on consolidating the collagen remodeling that the earlier treatments initiated. Full collagen maturation continues for three to six months after the last treatment session as the fibroblasts continue producing and organizing new matrix.
No treatment eliminates stretch marks completely. The clinical expectation is significant reduction in visibility, improved skin texture, and better integration between the stretch mark zone and the surrounding skin. The 80 to 90 percent improvement rates in the clinical literature refer to measurable reduction in severity scores and patient-reported satisfaction, not complete erasure. This is the honest framing we use in consultations.

Skin Tone and Why It Matters for Stretch Mark Treatment in South Florida
Miami and Doral have one of the highest concentrations of Fitzpatrick III-VI patients in the United States. This demographic reality shapes every protocol decision we make for stretch mark treatment. Post-inflammatory hyperpigmentation is a real risk for darker skin tones with any treatment that involves controlled skin injury, including microneedling, RF microneedling, and fractional laser. That risk does not mean these modalities cannot be used safely. It means they require adjusted parameters, longer spacing between sessions, and consistent sun protection to avoid triggering a hyperpigmentation response in the tissue surrounding the treated area.
For stretch mark treatment specifically, PDRN mesotherapy is often the lowest-risk starting point for Fitzpatrick IV, V, and VI patients because it delivers the regenerative stimulus without the thermal or mechanical component that creates hyperpigmentation risk. We use PDRN as the foundation of the protocol and introduce microneedling or laser at reduced settings and increased intervals once we have assessed how the skin responds. South Florida patients also deal with year-round UV exposure, which means sun protection between sessions is a clinical requirement. Laser-treated and microneedled skin is significantly more vulnerable to UV-triggered hyperpigmentation in the weeks after treatment, and in a climate like Miami, that window requires active management. SPF 30 or higher, mineral formulations preferred, applied every morning starting three days after a session, is the standard protocol we give every patient regardless of skin tone, and it is especially non-negotiable for Fitzpatrick III and above. For more detail on how we approach laser and injectable treatments for darker skin tones, our guide to PDRN for neck lines and tech neck at Perfect B covers the clinical considerations for South Florida patients and how UV exposure and skin tone affect treatment spacing in an adjacent application.
Frequently Asked Questions
1. Is PDRN for stretch marks the same as a PDRN serum you can buy online?
No. PDRN serums sold as skincare products are applied topically to intact skin and cannot reach the reticular dermis where stretch marks form. Medical-grade PDRN treatment involves injecting or delivering purified polynucleotide solution directly into the dermis, where it can activate the A2A adenosine receptor pathway in fibroblasts and trigger collagen and elastin production, a mechanism we cover in detail in our full guide to salmon DNA PDRN facial therapy at Perfect B in Doral. The concentration, delivery depth, and mechanism are fundamentally different from a topical cosmetic product.
2. Does PDRN work on old white stretch marks or only new red ones?
PDRN works on both, but produces better results on striae rubrae (red, new stretch marks) than striae albae (white, mature ones). Red stretch marks still have active vascularity and inflammation, which gives the A2A receptor mechanism better conditions to work in. Mature white stretch marks respond more reliably when PDRN is combined with microneedling or RF microneedling, which provides the mechanical stimulus that atrophic tissue needs alongside the biochemical signal from PDRN. The combination protocol can produce significant improvement in striae albae, though more sessions are typically needed than for red marks.
3. How many PDRN sessions do stretch marks typically require?
Most stretch mark patients at Perfect B complete between three and nine months of treatment, with sessions scheduled every two to six weeks. Striae rubrae responding well to PDRN mesotherapy alone may see meaningful results in three to five sessions. Striae albae treated with the combination protocol typically require six to nine or more sessions for comparable improvement. The exact session count depends on the stage of the marks, the surface area, the skin tone, and how the tissue responds to early sessions.
4. Can PDRN be combined with the other stretch mark treatments at Perfect B?
Yes, and the combination protocols typically outperform single-modality approaches for stretch marks. At Perfect B, PDRN is incorporated into stretch mark protocols alongside Morpheus8 RF microneedling, SkinPen microneedling, and the ResurFx non-ablative fractional laser depending on what the specific case requires. PDRN provides the regenerative biological signal while the device-based treatments create the mechanical or thermal stimulus that activates the repair response in the dermis. The sequencing of modalities is determined at the consultation based on the stage of the striae and the patient’s skin tone.
5. Is PDRN treatment safe for darker skin tones?
PDRN mesotherapy alone is one of the lower-risk options for Fitzpatrick III-VI skin because it does not involve the thermal or mechanical component that creates post-inflammatory hyperpigmentation risk in darker tones. When PDRN is combined with microneedling or laser for mature stretch marks, those modalities require adjusted settings and longer spacing between sessions for darker skin. At Perfect B in Doral, we see a predominantly Fitzpatrick III-VI patient population and routinely adjust protocols accordingly. Sun protection between sessions is a clinical requirement, not optional, for anyone with Fitzpatrick III or above in the South Florida UV environment.
6. How soon can I see results after starting PDRN for stretch marks?
Most patients notice improvement in skin texture and hydration around the stretch marks within two to four weeks of the first session. Changes in the marks themselves, including reduced visibility, improved color blending, and better surface texture, typically become more apparent after the second or third treatment as the collagen remodeling process advances. The clinical studies that document 80 to 90 percent improvement rates measured outcomes at 20 weeks, which reflects the timeline for meaningful dermal remodeling rather than surface-level hydration changes. Full collagen maturation continues for three to six months after the last treatment session.
Closing: What This Means for Stretch Mark Patients at Perfect B
PDRN for stretch marks is not a replacement for the laser and RF microneedling modalities that have been the clinical standard for striae treatment. It is a biologic component that addresses the underlying regenerative deficit that those device-based treatments cannot fully resolve on their own. When PDRN is combined with the right mechanical or thermal stimulus at the right stage of the stretch marks, the combination consistently outperforms either treatment used in isolation, with a more complete collagen matrix and better overall skin quality as the outcome.
The consultation at Perfect B in Doral starts with an assessment of where your stretch marks are in their clinical progression, what your skin tone means for the protocol, and which combination of our available modalities gives you the best trajectory. PDRN may be part of that plan, or it may be one component alongside Morpheus8, SkinPen, or ResurFx depending on what your specific case needs. For other areas where we use PDRN at the clinic, including PDRN for under-eye circles, where the same A2A receptor mechanism addresses volume loss and crepey texture in the periorbital dermis, the approach is the same: clinical delivery to the tissue that needs repair, not a topical product, and a protocol built around what the evidence supports.
- 📍 Visit us at Perfect B, Doral FL, serving Miami and South Florida patients seeking PDRN stretch mark treatment.
- 📞 Call (786) 502-2260 or message us to schedule your stretch mark treatment consultation with a licensed medical provider.


