

Perfect B, Doral Fl. | 06.03.26 | 9 min read.
This content is for educational purposes only and does not substitute for personalized medical advice. Treatment protocols vary by individual. Consult a licensed medical provider before beginning any treatment.
The Rash Around Your Mouth That Won’t Respond to Acne Treatment
If you have been treating a rash around your mouth with benzoyl peroxide, salicylic acid, or retinoids for weeks and it keeps coming back or getting worse, there is a real possibility that you do not have acne at all. Perioral dermatitis is one of the most consistently misdiagnosed skin conditions in clinical practice. It appears where acne appears, it looks like acne, and it frustrates patients the same way persistent acne does. But the cause, the mechanism, and the correct treatment are entirely different. Every standard acne product you apply to perioral dermatitis can make it worse.
At Perfect B in Doral, FL, we see this pattern regularly. A patient comes in after months of treating a cluster of bumps around the chin, upper lip, or nose with acne products that are doing nothing. In some cases the rash has spread. The products were not failing because the acne was resistant. The diagnosis was simply wrong.

Key Takeaways
- Perioral dermatitis is not acne. It is a chronic inflammatory skin condition that affects the area around the mouth, nose, and sometimes the eyes. Its cause is distinct, and standard acne treatments do not work.
- The single fastest differentiator is the lip border. In perioral dermatitis, the skin immediately bordering the lips is always clear. This border-sparing pattern is not seen in acne.
- Topical corticosteroids are the most common cause, including OTC hydrocortisone creams that many patients apply thinking they are helping an inflammation. Stopping them is often the first treatment step.
- Acne products make it worse. Benzoyl peroxide, retinoids, and many acne cleansers irritate perioral dermatitis and can worsen the rash. Fluorinated toothpaste is a frequently overlooked trigger.
- Clinical treatment is effective and works quickly when the diagnosis is correct. Zero therapy combined with topical or oral antibiotics clears most cases within four to eight weeks.
What Is Perioral Dermatitis? The Condition Most Mistaken for Acne
Perioral dermatitis is a chronic inflammatory eruption that targets the skin around facial orifices, most commonly the mouth, nose, and occasionally the eyes. The word perioral means “around the mouth,” and that anatomical specificity is one of its diagnostic signatures. The rash consists of small papules and pustules, typically 1 to 2 millimeters, clustered in groups with mild redness in the surrounding skin. It can itch or burn, and unlike acne, it tends to cluster in a ring pattern rather than distributing broadly across the face.
The condition affects women between 25 and 45 most commonly, though men and children can develop it as well. In children, a granulomatous variant is more common, where the bumps appear yellowish rather than red. In adults, the clinical presentation is almost always the same: a band or cluster of small uniform papules in the perioral region that does not respond to acne treatment and recurs after apparent improvement.
A review published in StatPearls documenting the clinical features, differential diagnosis, and management of perioral dermatitis as a condition distinct from acne vulgaris that requires a different treatment approach and is commonly worsened by topical steroids captures the core of what we observe in clinical practice: the diagnosis is straightforward when the right clinical questions are asked, but it is routinely missed when providers default to treating visible facial bumps as acne.
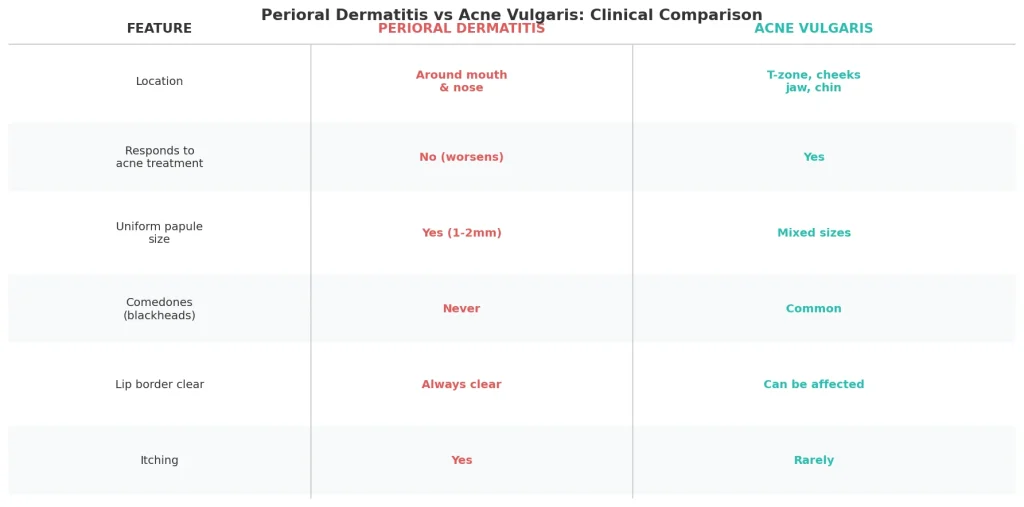
Perioral Dermatitis vs Acne: The 5 Clinical Differences That Matter
The distinction between perioral dermatitis and acne vulgaris is visible once you know what to look for. Most patients and many general practitioners miss it because they focus on what the rash looks like at a glance rather than its specific clinical markers. Here are the five features that separate them reliably.
1. Location: the perioral ring vs the sebaceous distribution
Perioral dermatitis forms a ring or band specifically around the mouth, nose, or eyes. The chin, upper lip line, and nasolabial folds are the most common sites. Acne vulgaris follows the sebaceous gland distribution of the face: T-zone, cheeks, jaw, and chin broadly. While both can appear on the chin and lower face, perioral dermatitis clusters in a tight perioral pattern rather than distributing diffusely across oily zones.
2. Comedones: present in acne, absent in perioral dermatitis
Acne vulgaris is defined in part by the presence of comedones, both open (blackheads) and closed (whiteheads). They form when sebum and dead skin cells plug a follicular opening. Perioral dermatitis never produces comedones. If a rash around the mouth includes blackheads or whiteheads, at least part of the condition is acne. A rash with no comedones at all and no response to acne treatment is strongly suspicious for perioral dermatitis.
3. Papule uniformity: mixed in acne, consistent in perioral dermatitis
Acne vulgaris presents with mixed morphology: papules, pustules, nodules, and cysts in the same zone, at different stages of development. Perioral dermatitis produces papules that are strikingly uniform in size (1 to 2mm) and stage, often appearing as a nearly identical cluster. When a patient shows a rash where every bump looks the same, that uniformity is a clinical signal toward perioral dermatitis.
4. Response to treatment: the clearest diagnostic clue
If a facial rash has been treated with benzoyl peroxide, salicylic acid, adapalene, or doxycycline for more than eight weeks without improvement, perioral dermatitis should be high on the differential. Standard acne treatments are simply ineffective against it. In cases where a patient was using topical corticosteroids, those treatments may have been actively perpetuating the condition. At Perfect B in Doral, treatment-resistant facial rashes that were previously managed as acne are among the most common presentations we re-evaluate from the ground up. → Read how Perfect B distinguishes between multiple causes of acne-like breakouts, including fungal folliculitis and bacterial acne, to ensure every treatment protocol matches the actual diagnosis.
5. Itch and burning: rare in acne, common in perioral dermatitis
Acne vulgaris rarely itches. Perioral dermatitis frequently does, and patients also report a burning sensation in the affected area. Most patients who have been treating the rash as acne report that they noticed the burning but attributed it to the products they were using. It is not always the products. The condition itself is responsible. Itching or burning in a perioral rash is a fast clinical flag toward perioral dermatitis.
The One Visual Clue That Changes the Diagnosis: Lip Border Sparing
There is a single visual marker in perioral dermatitis that, once you know it, makes the diagnosis immediately clear in most cases: the skin immediately bordering the lips (the vermilion border) is always clear. The rash clusters around the perioral area but stops before reaching the actual lip edge, leaving a narrow clear zone between the rash and the lip itself.
This lip border sparing is not seen in acne. Acne papules and pustules can appear on the chin, jaw, and perioral region without respecting any anatomical boundary. When a patient presents with a ring of papules around the mouth but the skin touching the lips is noticeably clear, that pattern is perioral dermatitis until proven otherwise. It is the fastest single clinical clue available without any testing, and it is the feature most patients have not been told about despite having seen multiple providers. At Perfect B in Doral, pointing this out to patients during the first consultation is often the moment they understand why nothing they tried before worked.
What Triggers Perioral Dermatitis? The Surprising Causes
The most common cause of perioral dermatitis is topical corticosteroid use on the face. This includes prescription-strength steroids as well as OTC hydrocortisone creams that patients apply to reduce redness, thinking they are managing an inflammatory skin condition. The steroids provide temporary relief, which reinforces continued use, while simultaneously perpetuating and worsening the underlying dermatitis. This cycle is one of the main reasons patients present with months of worsening rash.
Beyond steroids, a number of less obvious triggers are well documented. Fluorinated toothpaste is one of the most overlooked. The fluoride compounds in many standard toothpastes can trigger or sustain perioral dermatitis in susceptible individuals. Patients who switch to non-fluorinated toothpaste during treatment frequently see faster improvement. Heavy face creams and occlusive moisturizers are another significant trigger, particularly in South Florida where patients layer SPF products, primers, and moisturizers in a hot and humid environment that already stresses the perioral skin. The combination of product load and heat is a meaningful contributing factor for our patient population in Doral and Miami.
Other documented triggers include: inhaled corticosteroids (for asthma), heavy foundation makeup, hormonal fluctuations, and certain sunscreens. Stress has also been proposed as a contributing factor, consistent with what we observe in our acne cluster, where cortisol elevation drives sebaceous activity broadly. → Read how cortisol and stress hormones drive facial skin inflammation and breakouts, and what Perfect B uses to address the hormonal component of treatment-resistant skin conditions.
Why Standard Acne Products Make Perioral Dermatitis Worse
This is not a subtle effect. The same products that treat acne vulgaris actively worsen perioral dermatitis in most patients. Understanding why helps explain why so many patients present after months of ineffective treatment with a rash that has spread.
Benzoyl peroxide kills bacteria through oxidation. Perioral dermatitis is not a bacterial infection in the same sense as acne vulgaris. Applying benzoyl peroxide disrupts the skin barrier in the perioral area, increases irritation, and can worsen the inflammatory response without addressing the actual cause. Retinoids work in acne by regulating cell turnover and reducing comedone formation. Perioral dermatitis has no comedones. Retinoid application in this context irritates already compromised perioral skin without targeting the pathology. Salicylic acid cleansers are exfoliating agents appropriate for oily, comedone-prone acne skin. They are too stripping for the perioral dermatitis presentation and will increase irritation.
The most damaging product class is topical corticosteroids, including hydrocortisone. Patients commonly apply 1% hydrocortisone cream to calm what appears to be an inflammatory rash, and the steroid provides temporary visible improvement. But it does not resolve the dermatitis. It suppresses the visible symptoms while allowing the underlying inflammatory process to deepen. When the steroid is stopped, the rash returns worse than before. This creates the cycle described in the next section. → Read how Perfect B explains the mechanism of skin worsening before improvement in inflammatory skin conditions, and how to distinguish a productive reaction from a sign that treatment should change.
The Rebound Effect: Why Stopping the Steroid Feels Like It’s Getting Worse
One of the most important clinical concepts in perioral dermatitis management is what happens when a patient stops topical corticosteroid use. Within two to five days, the rash flares significantly. The papules multiply, redness increases, and the condition looks and feels worse than before the steroid was ever applied. This is the rebound or withdrawal effect, and it is the reason many patients restart the corticosteroid immediately, concluding that they need it to control the rash.
They do not need it. The flare is the expected response to steroid withdrawal, not evidence that the skin cannot improve without the medication. The steroid has been suppressing symptoms while the underlying inflammation continued. Stopping it allows the full extent of that inflammation to surface temporarily. If the patient holds course and avoids reapplication, the rash typically peaks within the first week and then begins to improve as the skin adjusts to the withdrawal. This process, often called “zero therapy” by dermatologists, requires the patient to tolerate a temporary worsening before real recovery begins.
At Perfect B, we explain this timeline explicitly before any patient stops corticosteroid use. The single most common reason perioral dermatitis does not resolve is the rebound cycle: stop, worsen, restart, brief relief, stop again, worsen again. Breaking that cycle requires understanding that the worsening is part of recovery, not a sign of failure. Clinical support during this phase, including topical or oral antibiotic coverage, significantly reduces the discomfort of the withdrawal period.

What Clinical Treatment of Perioral Dermatitis Actually Involves
Treatment of perioral dermatitis begins with elimination. Before any prescription agent is introduced, the triggering factors are removed: topical corticosteroids, heavy face creams, fluorinated toothpaste, occlusive sunscreens, and any other product that may be sustaining the inflammatory cycle. This zero therapy phase is the foundation of treatment. In mild cases, trigger elimination alone is sufficient to resolve the condition over several weeks.
For moderate to severe presentations, topical antibiotic agents are added. Metronidazole gel or cream applied twice daily is the most commonly used topical treatment. It does not cause the irritation that acne products do and is well tolerated by perioral skin. Topical erythromycin or azelaic acid are alternatives when metronidazole is not available or tolerated. These agents reduce the inflammatory response without disrupting the skin barrier in the way that benzoyl peroxide or retinoids would.
For persistent or widespread perioral dermatitis, oral antibiotics are effective. Doxycycline at low dose (anti-inflammatory, not antimicrobial) is the most commonly prescribed agent, typically for six to twelve weeks. A clinical study published in the Journal of the American Academy of Dermatology documenting that low-dose doxycycline produces significant improvement in perioral dermatitis within eight weeks without the side effects associated with full antimicrobial dosing reflects the standard of care currently in use. Most patients see meaningful improvement within three to four weeks of starting oral treatment, with full clearance by eight to twelve weeks.
Perioral Dermatitis vs Rosacea: When the Confusion Goes Further
Perioral dermatitis is most commonly confused with acne, but a significant subset of patients are also told they have rosacea. The distinction matters because rosacea management involves vasodilatory triggers (heat, alcohol, spice) and topical agents like metronidazole or azelaic acid that do overlap with perioral dermatitis treatment, but the underlying condition and long-term management are different.
Rosacea presents with persistent central facial redness, flushing, telangiectasias (visible broken capillaries), and inflammatory papules distributed across the nose, cheeks, forehead, and chin broadly. It typically does not cluster exclusively around the mouth the way perioral dermatitis does. Rosacea rarely shows the lip border sparing that characterizes perioral dermatitis. And rosacea is a chronic vascular condition that can be managed but not eliminated, while perioral dermatitis can fully resolve with correct treatment and trigger avoidance. Misdiagnosing perioral dermatitis as rosacea and treating with vasoconstrictors or long-term topical steroids for redness will perpetuate the perioral condition rather than resolve it. The clinical picture of both can also coexist in the same patient, in which case each component requires targeted management.

Frequently Asked Questions
1. How do I know if I have perioral dermatitis or acne?
The fastest clinical questions are: Is the rash exclusively around the mouth, nose, or eyes? Is the skin immediately bordering the lips clear (lip border sparing)? Are there no blackheads or whiteheads? Has standard acne treatment failed to improve it? Does it itch or burn? If the answers to most of these point toward perioral dermatitis, a clinical evaluation will confirm it. A provider who examines the distribution, morphology, and treatment history can typically distinguish the two without laboratory testing.
2. Can perioral dermatitis go away on its own?
In some cases, particularly when the trigger (usually topical corticosteroids) is removed, mild perioral dermatitis can resolve without prescription treatment. But most moderate presentations require at minimum trigger elimination plus topical antibiotic. Left untreated or treated with the wrong products, perioral dermatitis can persist for months or years. Without identifying and removing the trigger, resolution is unlikely regardless of what topical agent is applied.
3. Does fluoride toothpaste really cause perioral dermatitis?
It is one of the most documented but least discussed triggers. Fluorinated compounds in standard toothpastes can sustain perioral dermatitis in predisposed individuals. Switching to a non-fluorinated toothpaste is typically one of the first recommendations in zero therapy. It does not cause perioral dermatitis in everyone who uses it, but in patients with active perioral dermatitis, continued use of fluorinated toothpaste can prevent resolution. If you have perioral dermatitis, switching toothpaste is worth trying and costs nothing.
4. Why does my perioral dermatitis get worse when I stop the hydrocortisone?
This is the rebound or withdrawal effect. Topical corticosteroids suppress the visible symptoms of perioral dermatitis while the underlying inflammation continues. When the steroid is stopped, the suppressed inflammation surfaces in full, causing a flare within two to five days. This is expected and temporary, not a sign that the skin cannot improve without the steroid. Restarting the corticosteroid at this point restarts the cycle. Clinical supervision during this phase helps patients tolerate the withdrawal period and provides antibiotic coverage to support resolution.
5. How long does perioral dermatitis take to clear?
With correct treatment (trigger removal plus topical or oral antibiotic), most patients see meaningful improvement within three to four weeks and full clearance within eight to twelve weeks. Mild cases with a clear single trigger, such as a topical steroid that is stopped and replaced with topical metronidazole, can clear faster. Cases with multiple triggers or a long history of mismanagement may take longer to fully resolve. Recurrence is possible if triggers are reintroduced, particularly topical steroid use.
6. Can perioral dermatitis turn into rosacea?
Cleveland Clinic documents that some perioral dermatitis cases that recur can eventually transition toward rosacea. The two conditions share some overlapping features: perioral dermatitis around the nose can involve redness and papules that resemble early rosacea. Whether this represents true conversion or a diagnostic shift is debated. What is consistent in the literature is that chronic, poorly managed perioral dermatitis with repeated steroid cycles increases the likelihood of persistent facial inflammation that over time may present as rosacea. Contact us at (786) 502-2260 to discuss your specific presentation and get a clear diagnosis before the condition progresses.
Closing: Getting the Diagnosis Right Is the Entire Treatment
Perioral dermatitis is not a rare condition. It is a common, well-characterized, fully treatable skin condition that is misdiagnosed as acne with sufficient frequency that many patients spend months applying the exact products that sustain or worsen it. The clinical picture is distinctive once the right markers are examined: perioral distribution, lip border sparing, absence of comedones, treatment resistance, and the history of topical steroid use. When those features are present together, the diagnosis is clear and the treatment pathway is direct.
At Perfect B in Doral, FL, we build the evaluation of perioral dermatitis into every consultation where a patient presents with a treatment-resistant perioral rash, because the cost of a missed diagnosis is months of ineffective treatment and a worsening cycle that is entirely avoidable. Getting the diagnosis right on the first visit changes everything. → Schedule a consultation at Perfect B in Doral, FL to have your skin evaluated by a licensed medical provider who distinguishes between perioral dermatitis, acne, and rosacea before designing a treatment protocol.
- 📍 Visit us at Perfect B, Doral FL, serving Miami and South Florida patients seeking perioral dermatitis diagnosis and treatment.
- 📞 Call or message us at (786) 502-2260 to schedule your skin evaluation consultation with a licensed medical provider.


