

Perfect B, Doral Fl. | 05.25.26 | 12 min read.
This content is for educational purposes only and does not constitute medical advice. BPC-157 and TB-500 are 503A compounded peptides administered under licensed medical supervision at Perfect B. All protocols are individualized at APRN intake. Results vary by patient, indication, and protocol adherence.
Skip Ahead to the Perfect B Peptide Protocol Tool. See Reconstitution, Daily Units, and Cycle Structure.
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida.
Answer 6 questions and see what patients with similar goals are running: which peptides they use, typical dosing, injection schedule, reconstitution steps, cycle length, and when they pause.
BPC-157 vs TB-500: The Question Everyone Gets Wrong
Most patients searching bpc-157 vs tb-500 assume they are choosing between two versions of the same thing. They are not. BPC-157 and TB-500 are not competing recovery peptides. They are complementary compounds that address different phases of the same repair process. BPC-157 repairs tissue at a specific location. TB-500 resets the inflammatory environment throughout the body. The injury pattern, not personal preference, determines which one makes clinical sense. At Perfect B in Doral, that determination happens at APRN intake, not by reading a forum post.
What the top-ranking competitors on this topic get wrong is treating this as a ranking exercise. TB-500 wins for systemic injuries. BPC-157 wins for localized injuries. The real question is what your specific injury picture looks like, and whether one peptide, the other, or the Wolverine Stack combining both, matches that picture.
Key Takeaways: BPC-157 vs TB-500
- BPC-157 is a localized repair peptide: derived from a protective protein in gastric juice, it promotes angiogenesis and collagen synthesis at the injection site, making it most effective when the injury is identifiable and accessible.
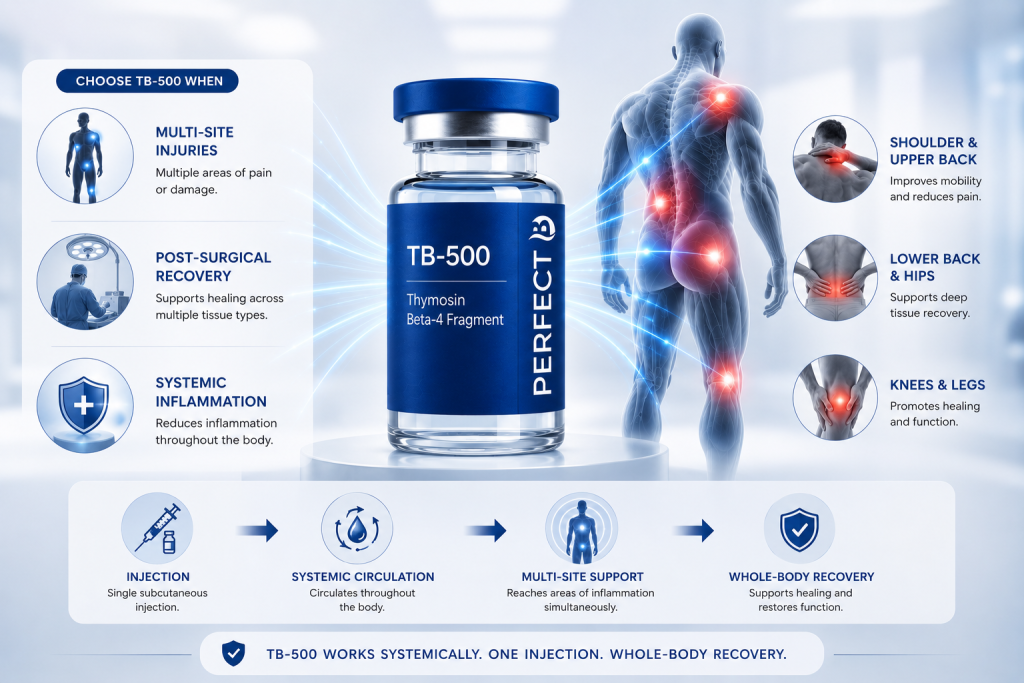
- TB-500 is a systemic recovery peptide: a synthetic fragment of Thymosin Beta-4, it circulates throughout the body to reduce inflammation, improve cell migration, and support recovery across multiple tissue types simultaneously.
- The selection criterion is injury pattern: single-site, localized damage responds best to BPC-157. Multi-site, post-surgical, or diffuse inflammatory presentations respond better to TB-500.
- The Wolverine Stack combines both: at $795 per cycle at Perfect B, the combination addresses both local repair and systemic inflammation when both are present, and the two peptides must be kept in separate vials, never mixed.
- Source matters as much as selection: both peptides are available as 503A compounded medications from licensed pharmacies or as unregulated research chemicals online. The difference in purity, dosing accuracy, and safety oversight is not a minor distinction.

South Florida patients researching both sides of this comparison typically also review the BPC-157 before and after results at Perfect B and the TB-500 benefits overview covering what this systemic recovery peptide does and who it is for.
What Does BPC-157 Actually Do at the Cellular Level?
BPC-157, short for Body Protective Compound 157, is a synthetic peptide derived from a protein found in human gastric juice. The origin is clinically significant: the gastric lining regenerates continuously despite exposure to acid and mechanical stress, and the peptide responsible for that regeneration turned out to be stable enough to isolate and study. What BPC-157 does at the tissue level is promote angiogenesis, the formation of new blood vessels into damaged tissue, and it activates growth hormone receptors in tendon fibroblasts, which accelerates collagen synthesis at the repair site.
The practical consequence of this mechanism is that BPC-157 works best when it can physically reach the target tissue. Subcutaneous injection near the injury site is the standard administration method for musculoskeletal indications because proximity to the damaged tissue maximizes the local angiogenic effect. For gastrointestinal indications, systemic or oral administration is appropriate because the entire gut is the target. BPC-157 loses its advantage when the injury is too distributed for a single injection site to cover.
What Does TB-500 Actually Do at the Cellular Level?
TB-500 is a synthetic version of a fragment of Thymosin Beta-4, a protein present at high concentrations throughout human tissue that plays a central role in cell migration, angiogenesis, and the regulation of inflammation. The key mechanical difference from BPC-157 is that TB-500 does not need to be injected near the injury. After subcutaneous administration, it circulates systemically, reaches multiple injury locations simultaneously, and modulates the inflammatory environment throughout the body rather than at a single point.
TB-500 works through actin regulation. Actin is a structural protein involved in cell movement, and TB-500 binds to actin monomers in a way that promotes cell migration into damaged tissue. This is the mechanism that makes TB-500 relevant to injuries that involve slow or stalled healing: when the local repair response has exhausted its resources, TB-500 recruits fresh cells from the surrounding tissue and circulatory system into the damage zone. At Perfect B in Doral, TB-500 is the peptide our providers reach for when a patient’s injury picture is too diffuse for a single-site injection to address completely.

The Mechanism Difference That Determines Your Protocol
The practical difference between bpc-157 vs tb-500 comes down to one question: is the injury localized enough that an injection can consistently reach it? If yes, BPC-157 gives you a direct activation signal at the repair site. If no, because the injury is spread across multiple locations, because inflammation is the primary barrier rather than tissue damage at one spot, or because the patient is post-surgical and every affected area cannot be injected individually, TB-500 addresses the problem at the systemic level that BPC-157 cannot reach.
A second distinction involves the anti-inflammatory pathway. BPC-157 modulates the nitric oxide system and suppresses specific inflammatory markers at the lesion site. TB-500 reduces systemic inflammation through Thymosin Beta-4’s broader role in immune regulation. Both reduce inflammation, but one does it at a point and one does it throughout the body. Patients with multiple sites of injury or chronic widespread inflammation need the systemic approach. Patients with one clearly defined injury need the local approach.
When to Choose BPC-157: The Single-Site Injury Profile
BPC-157 at $445 per cycle at Perfect B is the right choice when the injury is specific, accessible, and localized enough that subcutaneous injection can consistently reach the damaged tissue. The strongest clinical case for BPC-157 without TB-500 involves three presentations.
The first is single-site tendon or ligament injury: patellar tendinopathy, Achilles tendinopathy, plantar fasciitis, rotator cuff partial tears. The tissue is identifiable, the injection can be placed in proximity, and BPC-157’s direct activation of tendon fibroblasts and local angiogenesis addresses the biological bottleneck precisely. The second is gastrointestinal inflammation: BPC-157’s gastric origin gives it exceptional affinity for gut tissue, and the preclinical data on gut permeability, mucosal repair, and intestinal motility is the strongest body of evidence for this compound. The third is single-joint inflammation in a patient who has already addressed systemic inflammation and needs targeted structural repair at one location.
When to Choose TB-500: Multi-Site, Post-Surgical, and Systemic Recovery
TB-500 is the right choice when the recovery picture involves more than one location or when systemic inflammation is the primary barrier to healing. Post-surgical recovery affecting multiple tissue types, chronic widespread inflammation, and patients whose primary complaint is global stiffness and reduced range of motion that has not improved with localized treatment all fit the TB-500 indication.
The South Florida patient population at Perfect B in Doral includes a significant proportion of active adults over 45 who present with cumulative damage from years of activity, prior surgeries, and age-related tissue changes. These patients rarely have one discrete injury. They have patterns of damage across multiple joints and soft tissue areas that a single injection site cannot address. One subcutaneous TB-500 injection, anywhere on the abdomen, begins circulating to every site of inflammation in the body simultaneously. That systemic reach is what makes it the right choice for complex presentations where the injury picture is too diffuse for BPC-157 to resolve alone.
BPC-157 vs TB-500 for Tendon Repair: What the Research Shows
Tendon repair is the most frequently cited application for both peptides. The research supports each one for different aspects of that repair process. BPC-157 has been studied in tendon transection models with consistent findings: accelerated collagen synthesis, improved tensile strength at the repair site, and faster return of functional loading. A 2014 study in the Journal of Physiology and Pharmacology documenting BPC-157 and accelerated tendon healing with improved collagen fiber architecture. The localized mechanism explains the result: BPC-157 activates the fibroblasts that produce tendon collagen directly at the repair site.
TB-500 contributes to tendon repair through a different and complementary pathway. By promoting actin polymerization and cell migration, TB-500 moves repair cells from the surrounding tissue into the damaged tendon. This is particularly relevant in chronic tendinopathy, where the local repair response has stalled. A review in the Annals of the New York Academy of Sciences on Thymosin Beta-4 mechanisms in tissue repair and regeneration. The combination of both peptides addresses the complete repair sequence: TB-500 recruits cells systemically, BPC-157 activates them locally. In tendon cases where both local activation and systemic recruitment are needed, the Wolverine Stack addresses both simultaneously.
The Wolverine Stack: When Combining Both Makes Clinical Sense (And Why They Cannot Go in the Same Vial)
The Wolverine Stack, the combination of BPC-157 and TB-500, is the most requested recovery protocol among patients at Perfect B in Doral who have researched peptide therapy before their first appointment. At $795 per cycle, the stack addresses both local tissue repair and systemic inflammation simultaneously, and the clinical rationale is straightforward: the two peptides work through non-overlapping mechanisms that produce additive effects when both are present.
One critical detail that most online resources omit: BPC-157 and TB-500 must be administered from separate vials. They cannot be mixed into the same syringe or combined in the same vial. Mixing them creates stability and degradation risks that eliminate the clinical benefit of either compound. The correct protocol involves separate injections at separate sites, typically the same day or as directed by the prescribing APRN. This is a detail that matters and one that distinguishes a supervised clinical protocol from a self-administered one. → Read the Wolverine Stack protocol at Perfect B in Doral
Not sure which BPC-157 or TB-500 protocol fits your recovery goal?
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida. Answer 6 questions and see which protocol patients with similar goals chose: single peptide at $445, Wolverine Stack at $795, or a custom multi-peptide cycle.
Oral vs Injectable: What Influencers Will Not Tell You
Both BPC-157 and TB-500 are available in oral capsule form from research chemical suppliers. The reality of oral administration for musculoskeletal indications is straightforward: the peptide disperses through the digestive system before it reaches the injury site, and what arrives at a tendon or joint after that journey is a fraction of what a subcutaneous injection placed near the tissue delivers. For gastrointestinal indications, oral BPC-157 is appropriate because the gut is the target and the peptide does not need to travel further. For everything else, injection is the clinically validated route.
The oral capsule market exists largely because it is easier to sell and easier to self-administer without medical oversight. The price points are lower, the shipping is easier, and there is no injection anxiety. These are not clinical arguments. They are commercial arguments. At Perfect B in Doral, peptide protocols use injectable 503A compounded medications because the evidence base for musculoskeletal healing was built on injectable administration, and the clinical outcomes reflect that.
Compounding Pharmacy vs Online: The Safety Question No One Addresses
The peptide market has two supply chains. The first is 503A compounding pharmacies, licensed healthcare facilities that produce medications to individual prescriptions under pharmaceutical-grade standards, with purity testing, sterility protocols, and regulatory oversight. The second is research chemical suppliers, which operate outside pharmaceutical regulation and sell peptides as compounds “not for human use” to avoid FDA oversight.
The difference in product quality between these two channels is not theoretical. Independent testing of research-grade peptides purchased online has found purity levels ranging from below 50% to over 100% of stated concentration, along with bacterial endotoxin contamination and incorrect peptide sequences. A patient injecting a compound of unknown purity at an unknown concentration is not running a self-directed protocol. They are running an uncontrolled experiment on their own tissue. Perfect B sources all BPC-157 and TB-500 from licensed 503A compounding pharmacies, and both peptides require a prescription and APRN evaluation before any protocol begins.

How Long Does Each Take to Work? The Realistic Timeline
BPC-157 localized effects typically appear within two to four weeks of consistent dosing. The peptide acts directly on fibroblasts at the repair site, and patients with tendinopathy generally report noticeable reduction in localized pain and improved range of motion within that window. Full structural repair, if imaging is used to assess it, typically requires eight to twelve weeks. TB-500 systemic effects develop over a longer arc. The initial inflammatory modulation begins within the first one to two weeks, but the functional changes, including improved flexibility, reduced global stiffness, and better circulation, accumulate over four to eight weeks as the compound’s systemic effects build through repeated dosing.
Patients using the Wolverine Stack typically notice the BPC-157 effect first: localized pain reduction at the specific injury site, usually within two to three weeks. The TB-500 effect follows, with improvements in overall mobility and functional capacity emerging several weeks later. This sequential timeline is one reason the Wolverine Stack runs both peptides simultaneously rather than in sequence. The local repair signal from BPC-157 and the systemic recruitment signal from TB-500 complement each other in time rather than competing.
Not sure which BPC-157 or TB-500 protocol fits your recovery goal?
Perfect B’s peptide protocol tool is built on real clinical data from 2,000+ patients treated in South Florida. Answer 6 questions and see which protocol patients with similar goals chose: single peptide at $445, Wolverine Stack at $795, or a custom multi-peptide cycle.
Frequently Asked Questions
1. What is the main difference between BPC-157 and TB-500?
BPC-157 is a localized repair peptide that acts at the injection site to accelerate tendon, ligament, gut, and joint healing through direct fibroblast activation and angiogenesis. TB-500 is a systemic recovery peptide that circulates throughout the body to reduce inflammation, improve cell migration, and support recovery across multiple tissue types simultaneously. The right choice depends on whether the injury is discrete and localized or diffuse and multi-site.
2. Can BPC-157 and TB-500 be mixed in the same vial?
No. BPC-157 and TB-500 must be kept in separate vials and administered as separate injections. Mixing them creates stability and degradation issues that compromise the efficacy of both compounds. The Wolverine Stack at Perfect B uses separate injections at separate sites, timed according to the protocol prescribed by the APRN at intake.
3. Which is better for tendon repair: BPC-157 or TB-500?
For a single discrete tendon injury with an identifiable injection site, BPC-157 is typically more effective because it activates the fibroblasts that produce collagen directly at the repair location. For chronic tendinopathy where local repair has stalled, or for a patient with multiple tendon and joint issues simultaneously, the Wolverine Stack provides both the local activation signal and the systemic cell recruitment signal needed to restart the healing process.
4. How much do BPC-157 and TB-500 cost at Perfect B?
At Perfect B in Doral, BPC-157 as a standalone protocol is priced at $445 per cycle. The Wolverine Stack combining BPC-157 and TB-500 is $795 per cycle. Both include 503A compounded medication from a licensed pharmacy, APRN supervision, dosing instructions, and follow-up. Pricing reflects a supervised clinical protocol, not a research chemical purchase.
5. Do I need a prescription for BPC-157 or TB-500 in Florida?
Yes. Both BPC-157 and TB-500 are compounded peptides that require a prescription from a licensed Florida medical provider. At Perfect B in Doral, all peptide protocols begin with an APRN intake evaluation. The provider reviews injury history, current presentation, and recovery goals before prescribing any compound.
6. Is oral BPC-157 as effective as injectable for tendon healing?
For gastrointestinal indications, oral BPC-157 is appropriate because the gut is the target. For tendon, ligament, and joint repair, subcutaneous injection near the target tissue produces significantly stronger local effects than oral administration. The peptide disperses through the digestive system before reaching musculoskeletal tissue, and the concentration arriving at the injury site through the oral route is a fraction of what an injection delivers directly.
7. What is the difference between 503A compounded peptides and research chemicals?
503A compounded peptides are produced by licensed pharmaceutical facilities to individual prescriptions, with purity testing, sterility protocols, and regulatory oversight. Research chemicals are sold outside pharmaceutical regulation and have been independently tested to show purity ranging from below 50% to over 100% of stated concentration, along with contamination risks. Perfect B sources all peptides from 503A compounding pharmacies, and a prescription and APRN evaluation are required before any protocol begins.
The Clinical Takeaway from Doral
The bpc-157 vs tb-500 question does not have a universal answer because it is the wrong question. The right question is what the injury picture looks like and which compound matches that picture. BPC-157 matches localized, high-specificity damage where injection proximity to the repair site is achievable. TB-500 matches diffuse, systemic, or multi-site presentations where local injection cannot reach the full extent of the problem. The Wolverine Stack matches presentations where both local activation and systemic modulation are needed at the same time.
What none of the forum posts and influencer videos address is that a supervised clinical protocol, starting with a full medical intake, using 503A compounded medication, and including follow-up to adjust the protocol as recovery progresses, produces consistently better outcomes than a self-administered protocol built from research chemicals purchased online. The compound matters. The source matters. The supervision matters. At Perfect B in Doral, those three factors are the starting point, not an afterthought.
📍 Perfect B | 8200 NW 41st St, Suite 100, Doral, FL 33166
📞 (786) 502-2260
→ View the peptide treatment plan at Perfect B in Doral
For the bigger picture, read how peptide therapy is delivered under medical supervision at our Doral clinic as part of a complete, individualized plan.


