

Perfect B, Doral FL. | 06.04.26 | 9 min read.
This content is for educational purposes only and does not constitute medical advice. PDRN treatment protocols require clinical evaluation by a licensed medical provider. Consult a qualified provider before beginning any injectable or regenerative treatment.
Why PDRN Generates So Much Confusion
PDRN went from surgical wound care to K-beauty serum in a single decade, and the marketing caught up faster than the patient education did. The result is a treatment that most people either overcredit or dismiss entirely. At Perfect B in Doral, FL, we use injectable PDRN as one of our primary regenerative tools. We hear the same misconceptions in consultations every week. This post addresses the seven most common ones directly, with the evidence behind each answer.

Key Takeaways
- PDRN has 40 years of clinical history in surgical and wound care medicine before it ever appeared in a skincare serum. The experimental label does not hold.
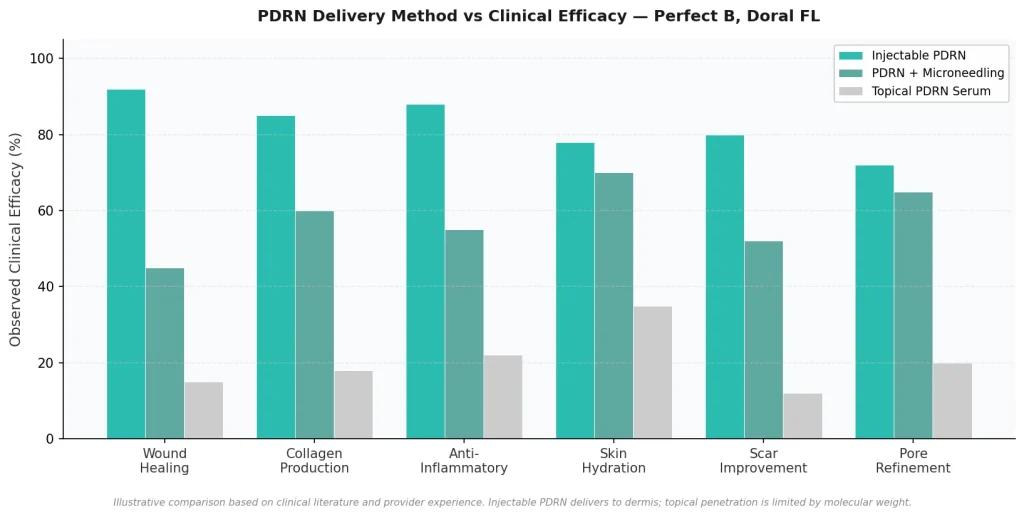
- Injectable and topical PDRN are not equivalent: Every clinical study showing significant tissue regeneration used intradermal injection. A serum sitting on the epidermis cannot replicate those results.
- PDRN is not a filler and does not add volume. It stimulates the skin’s own repair mechanisms through the A2A adenosine receptor pathway. The results are structural regeneration, not superficial filling.
- PDRN and PRP work through entirely different mechanisms. PDRN delivers a consistent, predictable biological signal. PRP potency varies with each patient’s platelet count.
- Results take time. Collagen remodeling and tissue regeneration are biological processes measured in weeks to months. Patients who expect immediate change are working with the wrong timeline.
Myth 1: “PDRN is just salmon DNA — it sounds experimental”
PDRN stands for polydeoxyribonucleotide. It is a chain of DNA fragments derived from salmon sperm, specifically selected because salmon DNA shares a high degree of structural similarity with human DNA. That similarity is not incidental. It is the reason PDRN integrates into skin cell signaling pathways without triggering an immune response, and it is what makes it clinically usable rather than experimental.
PDRN was first used in medicine in the 1980s for wound healing and tissue repair, long before aesthetic medicine adopted it. The primary mechanism of action is activation of the A2A adenosine receptor pathway, which regulates inflammation, cell proliferation, and angiogenesis. A comprehensive review of polydeoxyribonucleotide as a biological platform for accelerating wound healing confirms tissue regeneration through A2A receptor activation and the salvage pathway, with encouraging results in healing time and wound regeneration. This is not speculative biology. It is a well-characterized mechanism with four decades of clinical application behind it.
Myth 2: “The topical PDRN serum and the injectable do the same thing”
This is the most consequential myth in the PDRN space, and it is perpetuated primarily by skincare brands that cite injectable clinical studies to market topical products. The two delivery methods are not equivalent.
Injectable PDRN is delivered intradermally, directly into the dermis where collagen-producing fibroblasts and the repair cascade operate. The clinical evidence for injectable PDRN is robust: wound healing, tissue regeneration, collagen stimulation, and anti-inflammatory effects are all documented in peer-reviewed studies using intradermal delivery. Topical PDRN in a serum or cream sits on the epidermis. PDRN’s molecular weight of approximately 132,000 Daltons makes meaningful penetration through intact skin barriers extremely limited. There are almost no published clinical trials demonstrating the same regenerative outcomes from topical PDRN as from injectable PDRN.
The one exception is PDRN applied immediately after microneedling. When the SkinPen creates microchannels in the epidermis, PDRN applied topically in that window can enter the dermis through those channels. This is a specific delivery mechanism, and it is meaningfully different from applying a serum to intact skin. At Perfect B, PDRN stacking with microneedling is a deliberate clinical protocol, not a facial treatment. → The full explanation of what PDRN does at the cellular level and how it differs from other treatments is covered in the PDRN treatment guide at Perfect B.
Myth 3: “PDRN works like a filler”
Patients who come to consultations having researched both PDRN and hyaluronic acid fillers often ask which one adds more volume. The answer is that PDRN adds none. That is not a limitation. It is a fundamental difference in mechanism and clinical goal.
Dermal fillers work by physically occupying space under the skin. Hyaluronic acid draws water and creates immediate visible volume. The effect is instant and mechanical. PDRN works by signaling the skin’s repair systems to regenerate tissue. It activates fibroblasts, stimulates collagen synthesis, promotes angiogenesis, and reduces inflammation. The changes are gradual and structural rather than immediate and volumetric. A patient who wants immediate lift or volume is a filler candidate. A patient who wants progressive improvement in skin quality, hydration, texture, and laxity without added volume is a PDRN candidate. The two treatments serve different goals, and in many patients they are used together in a complementary protocol.
Myth 4: “PDRN is the same as PRP”
Both PDRN and PRP are biological injectables used in regenerative aesthetic medicine. That is where the similarity ends. The mechanisms, the variability, and the clinical predictability of the two treatments are fundamentally different.
PRP, platelet-rich plasma, is made from the patient’s own blood. It requires a blood draw, centrifugation, and preparation before each session. Its potency depends directly on the individual patient’s platelet concentration, which varies significantly between people. Two patients doing the same PRP protocol will receive treatments with different growth factor levels based on their own biology. PDRN, by contrast, delivers a consistent and standardized biological signal with every treatment. There is no blood draw required. The dose is predictable. The A2A adenosine receptor activation mechanism is the same regardless of which patient is receiving it. At Perfect B, PDRN is our primary regenerative injectable specifically because of this consistency. For patients with Fitzpatrick III to V skin types, the anti-inflammatory pathway of PDRN also makes it safer and more predictable than PRP in certain clinical contexts. → The full clinical comparison of PDRN and PRP, including which treatment fits which patient profile, is covered in the PDRN vs PRP guide at Perfect B.

Myth 5: “PDRN results are immediate”
Some patients notice improved skin luminosity and hydration within a few days after their first session. That early change is real, and it reflects the anti-inflammatory and hydration effects of PDRN at work. But it is not the result. It is the beginning of a process.
The regenerative outcomes of PDRN, including measurable improvement in skin laxity, texture, fine lines, and scar quality, are produced by the collagen remodeling and tissue regeneration cycle that PDRN triggers. That cycle operates on a biological timeline. Fibroblast activation accelerates collagen production during the weeks following each session. The new collagen matures and reorganizes progressively over 2 to 4 months. The most significant visible improvement in structural skin quality typically appears between the 6 and 12 week mark after a series of sessions, and continues to develop through month 4 to 6 as collagen type III is replaced by stronger collagen type I. Patients who come for one session and evaluate results at 10 days are measuring the wrong point on the curve.
Myth 6: “PDRN has no real clinical evidence”
This myth is the inverse of myth 2. Some patients who have read skeptical beauty media pieces come in having concluded that PDRN is unproven. What those articles are actually describing, accurately, is the limited clinical evidence for topical PDRN serums on intact skin. Injectable PDRN has a substantial and well-documented evidence base.
A study on PDRN’s effects in human skin keratinocytes and fibroblasts documents the A2A receptor binding mechanism, PDRN’s inhibition of inflammatory cytokines including IL-1 beta, IL-6, and TNF-alpha, and its stimulation of nucleic acid synthesis through the salvage pathway to support DNA formation and cell regeneration. The wound healing literature is particularly robust. Studies on diabetic ulcers, skin grafts, and post-surgical recovery consistently show that intradermal PDRN accelerates healing, reduces inflammation, and improves tissue quality compared to controls. The aesthetic medicine evidence built on that foundation. The distinction that matters is delivery method. Injectable evidence is strong. Topical evidence for intact skin is limited. The claim that PDRN has no evidence conflates the two.
Myth 7: “Any clinic that offers PDRN will give you the same result”
The ingredient is consistent. The clinical execution is not. PDRN outcomes vary significantly based on injection technique, depth, dosing, session spacing, and whether the treatment is matched to the patient’s actual skin concern and clinical profile.
At Perfect B, all PDRN treatments begin with an APRN consultation to assess skin type, Fitzpatrick classification, current concerns, and whether PDRN is the right primary treatment or should be stacked with microneedling, exosomes, or other protocols. For South Florida patients with Fitzpatrick III to VI skin, this assessment includes specific evaluation of post-inflammatory hyperpigmentation risk and anti-inflammatory protocol design. A PDRN facial booked at a spa by an aesthetician who cannot inject and a PDRN injection protocol administered by an APRN at a medical aesthetic clinic are not the same procedure. Treating them as equivalent based on the ingredient name produces mismatched expectations and suboptimal outcomes. → The complete PDRN safety guide at Perfect B, including the six patient groups we screen before approving treatment and the difference between topical and injectable safety profiles, is available here.

Frequently Asked Questions
1. Is PDRN FDA-approved for cosmetic use in the United States?
Topical PDRN is legal as a cosmetic ingredient in the US. Injectable PDRN for cosmetic and aesthetic use is administered off-label in the United States, as no injectable PDRN product currently holds FDA cosmetic approval. This is different from being unsafe. Many well-established aesthetic treatments are administered off-label. At Perfect B, all injectable PDRN treatments are performed by a licensed APRN with full clinical disclosure of regulatory status.
2. Does PDRN work for acne scars?
Yes, when delivered correctly. Injectable PDRN stimulates collagen production in the dermis, which progressively improves the texture and depth of atrophic acne scars over a series of sessions. The results are most significant for rolling and shallow boxcar scars. Deep ice pick scars typically require a different primary approach. PDRN stacked with microneedling is one of the more effective protocols for moderate acne scarring because the microneedling creates direct dermal access for the PDRN and compounds the collagen stimulus. → See the PDRN before and after guide at Perfect B for result timelines and concern-specific outcomes.
3. How many PDRN sessions are needed?
Most treatment plans at Perfect B involve 3 to 4 sessions spaced 2 to 4 weeks apart for initial improvement, followed by maintenance sessions every 2 to 3 months depending on the patient’s goals and response. A single session produces early improvements in hydration and skin quality, but the structural regenerative outcomes of PDRN require a series to achieve meaningful and lasting change.
4. Is PDRN safe for darker skin tones?
Yes. PDRN’s anti-inflammatory mechanism actually makes it well-suited for Fitzpatrick III to VI skin types because it does not generate the inflammatory cascade that triggers post-inflammatory hyperpigmentation the way some other treatments can. At Perfect B, where the majority of patients present with Fitzpatrick III to VI skin, PDRN is frequently chosen over PRP specifically for this reason. Protocol modifications including pretreatment assessment and post-treatment brightening support are still used as standard practice.
5. Can I use a PDRN serum at home instead of getting injections?
Topical PDRN serums are safe and may offer some surface benefits including hydration support and mild anti-inflammatory effects. They are not a substitute for injectable PDRN for patients seeking regenerative skin improvement. The delivery problem is real: PDRN’s molecular weight limits penetration through intact skin, and the clinical studies showing meaningful tissue regeneration all used intradermal injection. A topical PDRN serum is a reasonable complement to an in-clinic injectable protocol. It is not a replacement for it.
The Clinical Bottom Line on PDRN
PDRN is a well-characterized regenerative compound with four decades of clinical use and a defined mechanism of action. The evidence is strong for injectable delivery and limited for topical delivery on intact skin. It is not a filler, not equivalent to PRP, and not a treatment where results arrive in the first 48 hours. Patients who understand what it actually does and commit to the treatment timeline are consistently satisfied with what injectable PDRN produces.
📍 Perfect B | 3905 NW 107th Ave, Suite 104, Doral FL 33178
📞 Call or message us at (786) 502-2260 to schedule your PDRN consultation with a licensed medical provider.
💳 Buy Now Pay Later: Cherry, Klarna, Afterpay, CareCredit


