

Perfect B, Doral Fl. | 05.22.26 | Rolling Scars Guide | 13 min read.
This article is for educational purposes only and does not substitute professional medical advice. Always consult a licensed medical provider before starting any acne scar treatment. Results vary by patient, scar depth, and skin type. It is worth knowing how acne scars are treated at Perfect B in Doral using the right techniques for rolling, boxcar, and icepick scars.
Rolling scars are the acne scar type that responds best to treatment when the approach matches the anatomy. At Perfect B in Doral, we see this scar type regularly in patients across South Florida, and the consistent clinical reality is this: scars that have not improved with microneedling or laser alone were almost always treated in the wrong order. The tethering band that pulls the skin down was never released first. Until it is, every resurfacing treatment is working against a structure that is still anchored below the surface.
This guide covers the anatomy, how the tethering mechanism works, why subcision has to come before everything else, and how Perfect B approaches rolling scar treatment for the South Florida patient population, which skews heavily toward Fitzpatrick III through VI skin tones where treatment sequencing and PIH risk management are particularly critical.
Key Takeaways on Rolling Scars
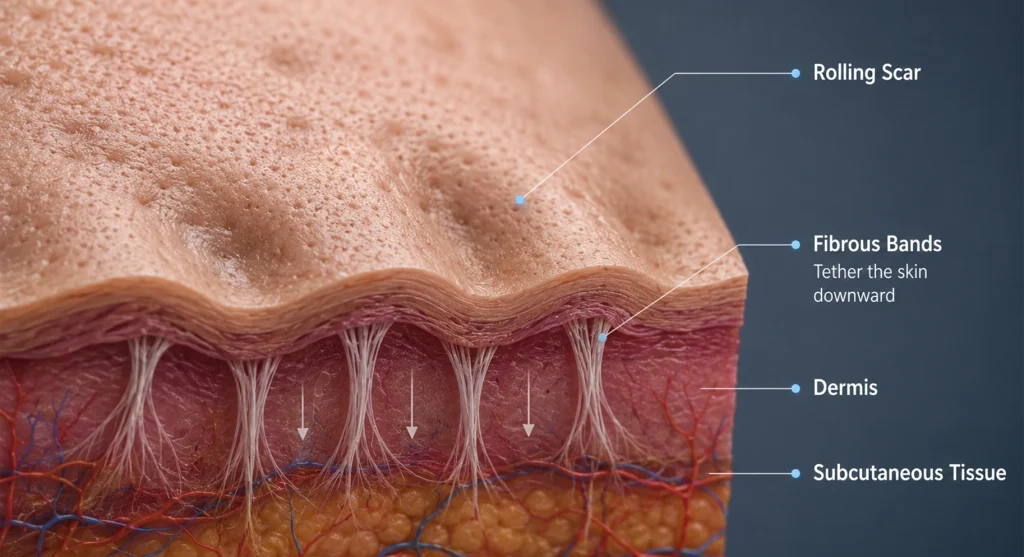
- Rolling scars are a tethering problem, not a surface problem: The wavy, undulating depressions are caused by fibrous bands that pull the epidermis downward toward the subcutaneous tissue. No surface treatment can release those bands. Subcision must come first.
- Subcision is Stage 1 at Perfect B: Every rolling scar protocol at our Doral clinic begins with subcision to release the fibers creating the depression before any resurfacing or remodeling is considered. Skipping this step produces partial, temporary results at best.
- Morpheus8 RF microneedling is Stage 2: After the tether is released, RF microneedling stimulates collagen remodeling from below to fill the depression. Morpheus8’s fractionated radiofrequency energy is delivered into the dermis at controlled depths, making it particularly well suited for the scar architecture of rolling scars.
- Skin tone changes the protocol: Patients with Fitzpatrick III through VI skin tones, which describes the majority of patients at our Doral clinic, require protocol adjustments to manage post-inflammatory hyperpigmentation (PIH) risk at each stage. The sequencing, energy settings, and recovery protocols are not interchangeable between skin tones.
- Rolling scars are the most treatable atrophic scar type: Unlike icepick scars, which are narrow and deep and require specialized evaluation, this scar type responds well to subcision combined with collagen-stimulating modalities. The anatomy, broad and shallow with sloping edges and a releasable tether, is accessible to staged treatment in a way that icepick and deep boxcar scars are not.
- Multiple sessions are required: Significant improvement typically requires 2 subcision sessions and 3 Morpheus8 sessions, followed by resurfacing and color correction as needed. Patients who expect results from a single session of any modality will be consistently disappointed.
What Rolling Scars Are and Why They Look the Way They Do
these scars are a type of atrophic acne scar characterized by broad, shallow depressions with sloping edges that give the skin a wavy, uneven appearance. They typically measure 4 to 5 millimeters or more in diameter and are most common on the cheeks, lower face, and jawline, where the skin is thicker and more susceptible to fibrous band formation during the healing process from severe inflammatory acne.
The appearance changes with lighting and skin tension. Under direct lighting, these scars can appear relatively subtle. Under raking or angled light, the undulations become much more pronounced. Patients often report that their scars look worse in certain lighting conditions, in photos, or when their skin is dehydrated. This is normal and reflects the topographical nature of the scarring rather than variation in the scar itself.
They are one of three main atrophic acne scar types, alongside icepick scars and boxcar scars. For a complete overview of all three types and how they differ in anatomy, depth, and treatment approach, see our clinical guide to the types of acne scars and how Perfect B identifies and treats each one. Understanding which scar type you have is the first step in building a realistic treatment plan. A plan designed for icepick scars will underperform on rolling scars. A plan targeting rolling scars without releasing the underlying tether will produce surface improvement over a structure still being pulled down from below.
How Rolling Scars Form: The Tethering Mechanism Explained
they form when severe inflammatory acne, particularly nodular or cystic acne that extends deep into the dermis, destroys the collagen architecture in the tissue below the skin surface. As the inflammation resolves and the tissue heals, fibrous bands form between the lower dermis and the subcutaneous fat. These bands tether the epidermis downward, creating the depression and undulation visible at the surface.
The tether is the defining anatomical feature of this scar type. It is also why it responds differently to treatment than other atrophic scar types. Icepick scars are narrow, deep channels that require targeted chemical or surgical intervention to destroy the scar epithelium. Boxcar scars have defined vertical walls and may require a combination of subcision and resurfacing to address both the tether and the edge geometry. they have a more accessible anatomy: the depression is broad, the edges slope, and the tether is subcutaneous rather than deep dermal, making it directly reachable by subcision.
The clinical literature supports this anatomy. A 2022 study published in the Journal of Drugs in Dermatology on combined treatment of rolling acne scars in ethnic skin demonstrated that combining tumescent subcision with erbium laser resurfacing and a 20% TCA peel produced significant improvement in Fitzpatrick III through VI patients, confirming that the release-first protocol with multimodal follow-up is both effective and safe for the skin types most common in South Florida.
Rolling Scars vs Boxcar Scars vs Icepick Scars: The Clinical Differences
Misidentifying scar type leads to mismatched treatment. At Perfect B in Doral, the APRN consultation classifies scar type before any treatment is selected, because the clinical approach for each type is fundamentally different.
- Rolling scars: Broad, shallow depressions with sloping edges and a subcutaneous tether. 4mm or wider. Most responsive to subcision plus collagen remodeling. Primary treatment: subcision first, then Morpheus8, then resurfacing as needed.
- Boxcar scars: Wide depressions with defined vertical walls and a flat base. Sharply demarcated edges that distinguish them from rolling scars on examination. Shallow boxcar scars respond well to RF microneedling. Deep boxcar scars with fibrous attachments may require subcision plus resurfacing. The treatment approach for boxcar anatomy differs significantly from rolling scars. For a full breakdown see our guide to boxcar scars and how their anatomy requires a different treatment approach than rolling scars.
- Icepick scars: Narrow, deep channels extending into the lower dermis. Small diameter (1-2mm) but very deep. Do not respond to surface resurfacing. Primary treatment: requires specialized clinical evaluation. At Perfect B, icepick scar cases are assessed individually at APRN consultation to determine the appropriate protocol. See our complete guide to icepick acne scars and why they require a different treatment approach than rolling or boxcar scars.
Many patients present with mixed scar types simultaneously. This is the most common presentation at Perfect B. The APRN consultation maps each scar type present, determines which is dominant, and sequences the treatment protocol accordingly.
Why Subcision Has to Come Before Everything Else
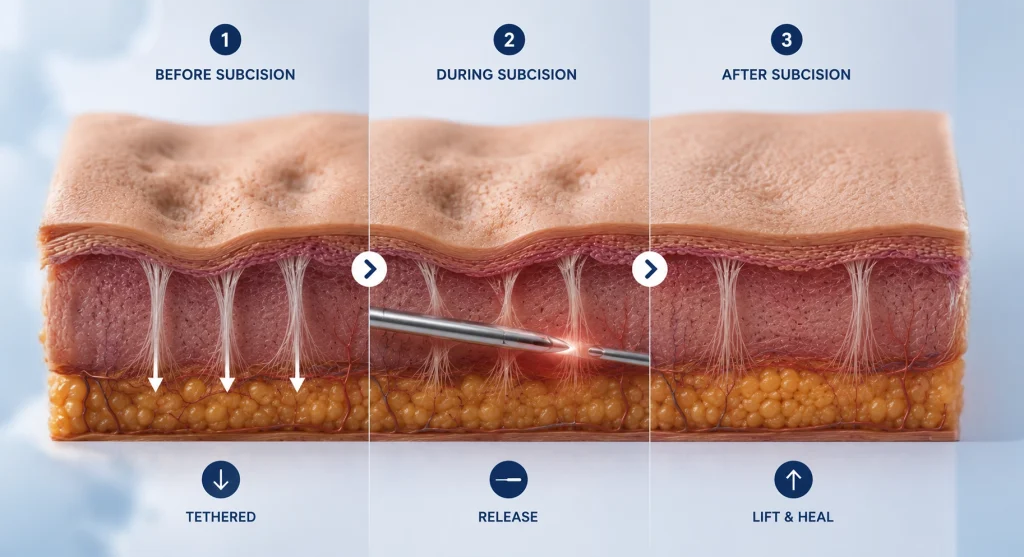
The reason subcision must come first is mechanical: as long as the fibrous band is intact, the skin is being pulled down toward the subcutaneous tissue. Any treatment applied to the surface or even to the dermis is working against an active downward force. Collagen remodeling from RF microneedling produces new collagen that fills from above and from within the dermis. If the tether is still pulling the epidermis downward, that new collagen is partially counteracted before the patient can see the benefit.
Subcision works by inserting a needle or cannula beneath the skin at the level of the subcutaneous fat and sweeping it to break the fibrous bands without removing them. The physical disruption of the tether releases the skin and allows it to return toward the surface. The procedure also creates a small controlled hematoma beneath the scar, which stimulates collagen synthesis as part of the healing response. This dual mechanism, mechanical release plus biological stimulation, is why subcision is the foundation of rolling scar treatment rather than an optional add-on.
At Perfect B in Doral, subcision for this scar type is performed as part of a staged treatment plan. Patients are counseled before the procedure that bruising and swelling are expected and are part of the healing process, not complications. The post-subcision period, typically 2 to 4 weeks, allows the initial healing response to stabilize before Morpheus8 RF microneedling is introduced for the remodeling phase.
Rolling Scars and RF Microneedling: What Morpheus8 Does After Subcision
Once subcision has released the tether, the second stage of rolling scar treatment at Perfect B is Morpheus8 radiofrequency microneedling. Morpheus8 delivers fractionated RF energy into the dermis at precise depths through microneedle arrays, stimulating fibroblast activity and new collagen synthesis throughout the scar tissue architecture.
For rolling scars specifically, the Morpheus8 protocol addresses two things that subcision alone does not fully resolve. First, it promotes organized collagen remodeling to fill the depression from within the dermis, rather than relying solely on the body’s unguided healing response after tether release. Second, it improves overall skin quality in the treated area, including texture, pore size, and skin firmness, which contributes to the visual improvement beyond the specific scar topography.
Morpheus8 is particularly well suited for this treatment in the South Florida patient demographic because its fractionated delivery and controlled depth settings make it appropriate for Fitzpatrick III through VI skin tones with a lower PIH risk profile than ablative laser resurfacing. For patients with darker skin tones, the ability to treat at depth while limiting surface thermal injury is clinically significant in managing the risk of post-inflammatory hyperpigmentation that can complicate acne scar treatment in this population.
acne scars in darker Skin Tones: What Changes at Perfect B in Doral
The majority of patients seeking rolling scar treatment at Perfect B present with Fitzpatrick III through VI skin tones, reflecting the South Florida demographic of Doral, which draws heavily from Hispanic, Latino, Caribbean, and Brazilian communities with medium to darker skin. For these patients, rolling scar treatment is effective, but the protocol requires specific adjustments that are not always addressed in general content about acne scar treatment.
The primary concern in darker skin tones is post-inflammatory hyperpigmentation (PIH). Any treatment that creates inflammation in the skin, including subcision, microneedling, and laser, carries a higher PIH risk in Fitzpatrick III through VI patients than in lighter skin tones. PIH produces dark patches that can persist for months and, if inadequately managed, can make the overall appearance of the skin worse than the scars being treated.
- Pre-treatment preparation: Patients with Fitzpatrick III-VI typically begin a pre-treatment protocol at Perfect B that includes melanocyte-stabilizing agents to reduce the skin’s inflammatory response before subcision. This preparation period reduces PIH risk during the treatment phases.
- Subcision settings and technique: Tumescent anesthesia during subcision reduces bleeding and bruising, which lowers the inflammatory stimulus and correspondingly reduces PIH risk. The technique and entry points are adjusted based on the patient’s specific scar anatomy and skin tone assessment at the APRN consultation.
- Morpheus8 parameters: Energy settings, needle depth, and pass counts are calibrated for Fitzpatrick classification. Higher energy settings that might be appropriate for Fitzpatrick I-II carry greater risk of thermal injury and PIH in darker skin tones and are not applied at the same parameters.
- Post-treatment protocol: Strict sun protection and melanocyte-stabilizing agents continue through the post-treatment period to prevent PIH from the healing response. Patients at Perfect B receive specific aftercare instructions calibrated to their skin tone.

How Many Sessions Does It Take to improve the appearance?
At Perfect B, the standard the standard protocol involves 2 subcision sessions and 3 Morpheus8 RF microneedling sessions as the core treatment sequence, followed by resurfacing and color correction stages as indicated. Sessions are spaced 4 to 6 weeks apart to allow the collagen remodeling response from each treatment to stabilize before the next session adds to it.
The improvement timeline follows the collagen remodeling cycle. Initial lifting of the depression can be visible within 4 to 6 weeks of the first subcision as the tether is released and the healing response begins. More significant improvement becomes apparent after the Morpheus8 sessions as new collagen fills the area that was previously tethered downward. The full result of the collagen remodeling from each session continues to develop for 3 to 6 months after the session, which is why the visual outcome at 6 months post-treatment is substantially better than at 6 weeks.
Patients with deeper or more fibrotic cases, particularly those with a long history of repeated cystic acne, may require additional sessions beyond the standard protocol. The APRN consultation at Perfect B assesses scar depth and fibrosis before projecting a realistic treatment course, and follow-up assessments after each session allow the protocol to be adjusted based on actual response rather than a fixed predetermined number of sessions.
Who Is a Candidate for Rolling Scar Treatment at Perfect B?
Rolling scar treatment at Perfect B is appropriate for patients who meet the following clinical criteria, assessed at the APRN intake consultation.
- Active acne must be controlled: Rolling scar treatment cannot be effective if new cystic acne lesions are forming in the same area. New inflammatory lesions create new tethering bands and undo the structural progress from treatment. Patients with active moderate to severe acne are referred for acne management before scar treatment begins.
- Realistic expectations about timeline: Rolling scar treatment produces cumulative improvement over a multi-month protocol. Patients who expect dramatic results from a single session or who want a 2-week recovery to a resolved appearance are not a good fit for what the treatment can actually deliver.
- Fitzpatrick assessment completed: All patients at Perfect B undergo Fitzpatrick classification at the APRN consultation. This determines the specific protocol parameters, pre-treatment preparation, and post-treatment care appropriate for their skin tone. Fitzpatrick III through VI patients require more preparation and more conservative treatment parameters, but the clinical outcomes are comparable to lighter skin tones when the protocol is properly adjusted.
- Rolling scar diagnosis confirmed: Subcision is specific to this scar anatomy. Applying subcision to icepick scars or boxcar scars without fibrotic attachments will not produce the same results and can create complications. The APRN consultation confirms scar classification before recommending subcision.
Rolling Scars Before and After: What Realistic Results Look Like
Before and after results from properly staged treatment for rolling scars are among the most visually compelling improvements in acne scar treatment. Because this anatomy is addressable at its root cause, the structural change from releasing the tether and stimulating collagen remodeling is genuine and lasting.
What realistic before and after results look like at Perfect B for rolling scars depends on the severity and depth of the scarring. Mild to moderate rolling scars typically show 60 to 80 percent improvement in overall skin topography after the full staged protocol. Severe scars with deep fibrosis and significant dermal destruction may improve 40 to 60 percent, leaving some residual texture improvement that would require additional sessions or adjunct modalities to address further.
The before and after timeline follows the treatment stages. The most visible improvement typically appears between months 4 and 6 of the protocol, after the collagen remodeling response from the Morpheus8 sessions has had time to mature. Patients who photograph their skin at 6 weeks and compare it to baseline often underestimate the total improvement because the full collagen response has not yet developed. The 6-month comparison is significantly more representative of the actual outcome.

Frequently Asked Questions About Rolling Scars
1. What are rolling scars?
Rolling scars are a type of atrophic acne scar caused by fibrous bands that tether the epidermis downward toward the subcutaneous tissue. They appear as broad, shallow depressions with sloping edges that give the skin an undulating, wavy appearance. They are most common on the cheeks and lower face, where the skin is thicker and more prone to fibrous band formation during healing from severe inflammatory acne.
2. What causes rolling scars?
they are caused by severe inflammatory acne, particularly nodular or cystic acne, that destroys the collagen in the deep dermis. As the inflammation resolves, fibrous bands form between the lower dermis and subcutaneous tissue. These bands tether the overlying skin downward, creating the depression. Factors that increase risk include genetic predisposition to scarring, delayed acne treatment, picking or squeezing acne lesions, and smoking.
3. Does subcision hurt?
Subcision is performed under local tumescent anesthesia at Perfect B, which significantly reduces discomfort during the procedure. Patients typically experience pressure and movement sensation rather than pain during the procedure itself. The post-procedure period involves bruising and mild swelling for 1 to 2 weeks, which is a normal part of the healing process. Most patients describe the recovery as more than expected based on the size of the procedure, but manageable with standard aftercare.
4. How many subcision sessions are needed for rolling scars?
At Perfect B, the standard protocol includes 2 subcision sessions spaced 4 to 6 weeks apart as part of the treatment sequence. Some patients with mild presentations and minimal fibrosis show sufficient tether release after one session. Patients with deeper fibrosis or more severe scarring may require a third session. The number of sessions is determined after the first subcision based on the observed tissue response at the follow-up assessment.
5. Can rolling scars be treated with microneedling alone?
Microneedling alone, without subcision first, produces limited results for rolling scars because the tethering bands remain intact. The collagen stimulated by microneedling partially counteracts the downward pull of the tether, producing some surface improvement but not addressing the structural cause of the depression. At Perfect B, Morpheus8 RF microneedling is always performed after subcision, not instead of it. Patients who have tried microneedling alone without satisfactory results often respond well to the subcision-first protocol.
6. Are rolling scars permanent?
these scars do not resolve on their own. Without treatment, the fibrous bands that cause them remain intact indefinitely. With properly staged treatment, rolling scars show significant structural improvement that is lasting. The collagen remodeling achieved through subcision plus Morpheus8 produces permanent changes to the scar architecture. New acne lesions in the same area can create new tethering bands, which is why active acne must be controlled before and during rolling scar treatment.
7. How long does it take to see results from rolling scar treatment?
Initial improvement from subcision is visible within 4 to 6 weeks as the tether is released and the healing response begins. Significant improvement from the collagen remodeling phase becomes apparent between months 3 and 6 of the protocol. The full result of the Morpheus8 sessions continues to develop for 3 to 6 months after the final session. Patients are counseled at Perfect B that the 6-month assessment is the most meaningful milestone for evaluating total improvement rather than the 6-week point.
8. What is the difference between rolling scars and boxcar scars?
they have sloping edges and a broad, shallow depression caused by subcutaneous fibrous tethering. Boxcar scars have defined, sharp vertical walls and a flat base. The edge geometry is the key visual distinction: rolling scars look like gradual undulations in the skin surface, while boxcar scars have punched-out edges that create a clear boundary between the scar floor and the surrounding skin. The two types may coexist in the same patient. Both respond to staged treatment, but the protocols differ in sequencing and the specific role of subcision in each case.
Closing: Release First, Then Remodel
Rolling scars respond to treatment in a way that directly matches the anatomy. The mechanism is a tether. The first intervention releases it. Everything after that builds on the structural change the release makes possible. Patients at Perfect B in Doral who follow the complete staged protocol consistently achieve meaningful improvement in skin topography, and those who previously tried resurfacing approaches without subcision first typically see substantially better results when the sequence is corrected.
The South Florida patient population, with its prevalence of Fitzpatrick III through VI skin tones, benefits from a clinic that has built its protocol around the specific requirements of those skin types. The PIH management, the pre-treatment preparation, and the calibrated Morpheus8 parameters are not generic. They are built for the patients we actually see at our Doral clinic.
📍 Perfect B | 8200 NW 41st St, Suite 100, Doral, FL 33166
📞 (786) 502-2260


