

Perfect B, Doral Fl. | 05.21.26 | 11 min read.
This article is for educational purposes only and does not substitute professional medical advice. Always consult a licensed medical provider before starting any acne scar treatment. For medically guided care, see how acne scars are treated at Perfect B in Doral using the right techniques for rolling, boxcar, and icepick scars. For more on this, see our guide to Raised Acne Scars: Treating Hypertrophic and Keloid Scars, and how it is evaluated and treated at Perfect B in Doral.
Boxcar scars are the acne scar type that most often gets misidentified. Because they sit wider and shallower than icepick scars, patients sometimes assume they will be easier to treat. The reality is more nuanced. Boxcar scars with defined vertical walls and fibrous attachments to the deeper dermis require a different clinical approach than superficial texture issues, and treatments designed for icepick scars, particularly TCA CROSS, do not work on boxcar anatomy and can make outcomes worse.
At Perfect B in Doral, every acne scar assessment begins with an APRN consultation that classifies scar type, depth, and skin tone before any treatment is selected. This guide covers what boxcar scars are, how they differ from other acne scar types, why TCA CROSS is not used for boxcar scars, and what clinical protocols are appropriate by depth and Fitzpatrick classification in South Florida.

Key Takeaways on Boxcar Scars
- Boxcar scars are wide with defined edges: They measure 1.5 to 4.0 mm across with vertical walls and a flat base, forming when severe inflammation destroys collagen in a defined dermal area.
- Shallow vs deep changes everything: Shallow boxcar scars (under 0.5mm) respond well to SkinPen microneedling and moderate-depth RF. Deep boxcar scars require deeper RF energy and may benefit from subcision to release fibrous attachments before surface remodeling can be effective.
- TCA CROSS is not for boxcar scars: TCA CROSS is a highly concentrated chemical applied to the narrow base of icepick scars to trigger focal collagen remodeling. Applied to the wide base of a boxcar scar, it produces diffuse damage without the controlled scarring response that makes it effective for icepick. It is not part of the boxcar treatment protocol at Perfect B.
- Morpheus8 RF is the primary clinical tool: RF microneedling with Morpheus8 delivers radiofrequency energy at controlled depths, stimulating collagen remodeling through the dermis and subdermis simultaneously with the mechanical microneedling effect.
- Subcision addresses fibrous bands: For boxcar scars with visible fibrosis pulling the base of the scar downward, subcision releases the fibrous attachment before surface remodeling begins, allowing the treated skin to rise and fill the depression more effectively.
- Fitzpatrick III-VI requires specific protocols: South Florida patients predominantly present with higher Fitzpatrick skin types that require calibrated RF settings and device parameters to minimize post-inflammatory hyperpigmentation risk during healing.
What Are Boxcar Scars? Anatomy of a Wide, Defined Depression
Boxcar scars are a subtype of atrophic acne scarring. Atrophic means the scar sits below the surrounding skin surface due to a loss of tissue, as opposed to hypertrophic or keloid scars which rise above the surface. Boxcar scars are defined by their specific geometry: a round or oval depression with vertical walls and a flat or slightly rounded base.
The defining measurements of a boxcar scar are a width of 1.5 to 4.0 mm and a depth ranging from 0.1 to 0.5 mm or more. The vertical wall angle is what distinguishes a boxcar scar from rolling scars, which have a gradual wave-like slope without defined edges. When you look at a boxcar scar in raking light, the defined shadow at the edge of the depression is the wall. When you look at a rolling scar, the shadow blends into the surrounding skin without a clear boundary.
Boxcar scars occur most commonly on the cheeks and temples, where the skin is thicker and cystic acne produces more significant dermal inflammation. They can occur on the chin and jaw as well, though cheek presentations are most frequent in the patient population at Perfect B in Doral.
Shallow vs Deep Boxcar Scars: Why the Distinction Changes Everything
The most clinically important distinction within boxcar scars is depth. Shallow boxcar scars measure under 0.5 mm and have intact dermis at their base. Deep boxcar scars extend beyond 0.5 mm and often have fibrous tissue tethering the base of the depression to the deeper dermis or subdermis.
This distinction determines what treatment can realistically achieve. Shallow boxcar scars respond well to surface-level collagen stimulation: SkinPen microneedling, medium-depth chemical peels, and lower-energy RF protocols can produce visible improvement over a series of sessions because the dermis at the base of the scar is structurally intact and capable of remodeling.
Deep boxcar scars with fibrous tethering present a different problem. The fibrous band pulls the base of the scar downward and holds it in position even as new collagen forms above it. In this case, stimulating surface collagen remodeling without first releasing the fibrous attachment produces incomplete results: the skin tightens and smooths around the depression but cannot rise to fill it because the tether remains. This is why subcision is indicated for deep boxcar scars before or alongside RF treatment, not as an optional add-on.
According to a review published in the Journal of Clinical and Aesthetic Dermatology, the treatment selection for atrophic acne scars must account for scar subtype and depth, as treatments effective for one subtype may be ineffective or harmful for another. At Perfect B, the APRN assesses scar depth and subtype at the intake consultation to build the appropriate protocol from the start.
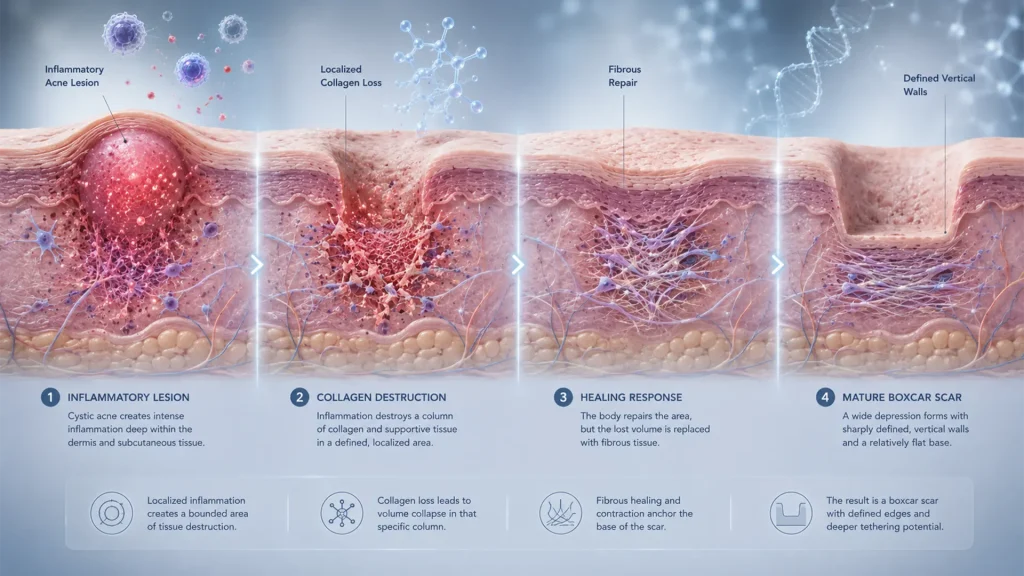
How Boxcar Scars Form: The Collagen Destruction That Creates Defined Walls
Boxcar scars form when a cystic or inflammatory acne lesion destroys collagen and subcutaneous tissue in a defined, localized area of the dermis. The inflammation does not spread diffusely the way rolling scar formation does; instead, it destroys a column of tissue with relatively sharp lateral boundaries, leaving intact dermis on either side of the lesion.
When the lesion heals, the skin above the destroyed tissue contracts downward without the collagen scaffold that would normally support it. The lateral boundaries of the original inflammatory zone become the walls of the scar. Because the destruction was bounded, the walls are defined and relatively steep. The base is flat where the collagen was lost rather than gradually sloped, which is why the shadow in raking light is sharp at the edge rather than gradual.
The deeper and more prolonged the inflammation, the more fibrous the healing response tends to be. Patients with a history of picking or squeezing cystic lesions, delayed treatment of active acne, or genetic tendencies toward fibrous healing are more likely to develop deep boxcar scars with fibrous tethering than patients whose acne was treated quickly and not manipulated.
Boxcar vs Icepick vs Rolling Scars: How to Tell the Difference
Patients often arrive at Perfect B unsure which scar types they have, which is common because many patients have more than one type simultaneously. The three main atrophic acne scar types have distinct visual and tactile characteristics that the APRN assesses at the consultation.
- Boxcar scars: Round or oval depressions, 1.5 to 4.0 mm wide, with vertical walls and a flat base. The edge shadow in raking light is defined. Predominant on cheeks and temples. Can be shallow or deep. Width is always greater than depth.
- Icepick scars: Narrow, deep, V-shaped channels extending from the surface into the dermis, typically under 2 mm wide. The shadow is deep and the channel is clearly visible on close examination. Cannot be compressed by lateral skin pressure. For a complete breakdown of icepick scar anatomy and treatment, see our icepick scar guide.
- Rolling scars: Broad, wave-like depressions with gradual sloping edges and no defined walls. Width is typically 4 to 5 mm or more with a much shallower depth relative to width. The shadow changes with facial movement. Rolling scars often feel soft and are compressible by lateral skin pressure, reflecting less fibrous tethering than deep boxcar scars.
A patient with all three types requires a layered approach where the treatment for each type is selected and sequenced appropriately. For a full overview of all acne scar types and how they are classified, see our guide to types of acne scars.
Why Boxcar Scars Are Harder to Treat Than They Look
The width of boxcar scars creates a visual impression that they should be easier to treat than narrow icepick scars. The logic seems intuitive: a wider opening should be easier to fill. The reality is that a wider scar requires more volumetric collagen replacement to produce a visible improvement at the surface, and the fibrous walls that define the scar boundary do not disappear with surface remodeling alone.
For shallow boxcar scars, a series of RF microneedling sessions can produce significant visible improvement because the collagen stimulation response is strong enough relative to the volume deficit. For deep boxcar scars with steep walls, the total volume of new collagen needed to fill the depression to the surface level is substantial, and the fibrous attachment at the base actively resists upward movement of the scar floor. This is why managing patient expectations about timeline and the number of sessions required is part of the intake consultation at Perfect B.
Patients who have seen minimal results from prior microneedling elsewhere often have deep boxcar scars where subcision was not performed before surface treatment. The microneedling stimulated collagen formation but the fibrous tether held the scar floor in place, making the improvement invisible at the surface despite real biological activity underneath.
What Does Not Work on Boxcar Scars (and What Is Only for Icepick)
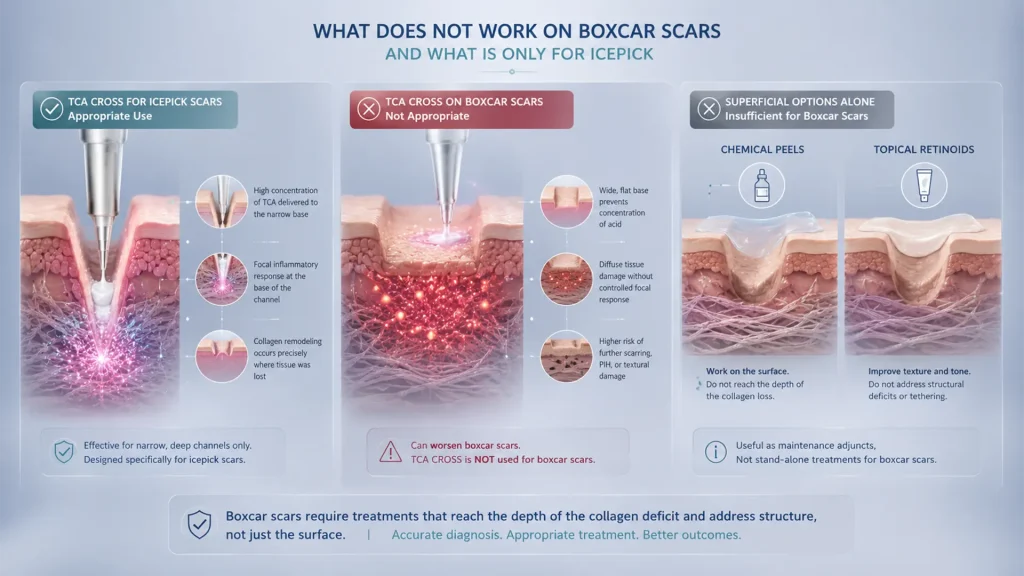
Understanding what not to use on boxcar scars is as important as knowing what works. The most common misapplication seen in patients who come to Perfect B after treatment elsewhere is TCA CROSS applied to boxcar scars.
TCA CROSS (Chemical Reconstruction of Skin Scars) involves applying a very high concentration of trichloroacetic acid to the precise base of a narrow icepick scar channel using a fine applicator. The focal chemical injury to the base of the narrow channel triggers an inflammatory response that produces collagen in the specific location where it was lost. The narrow geometry of the icepick channel concentrates the acid at the base, which is why the technique works for that scar type.
Boxcar scars have a wide, flat base. Applying TCA CROSS to a wide base does not concentrate the chemical in the way that produces the controlled focal response. Instead, it damages a broad area of tissue in a way that is more likely to produce further scarring, hyperpigmentation, or textural damage than improvement. TCA CROSS is specifically indicated for icepick scars and is not used for boxcar scars at Perfect B. If a provider recommends TCA CROSS for boxcar scars, that is a signal to get a second opinion.
Similarly, superficial chemical peels and topical retinoids used alone will not meaningfully improve established boxcar scars. They address surface texture and pigmentation but do not reach the depth at which the collagen deficit and fibrous tethering exist. They can be useful as maintenance adjuncts between clinical sessions but are not stand-alone treatments for moderate or deep boxcar scarring.
Clinical Treatments for Boxcar Scars: What the Evidence Shows
The clinical literature on atrophic acne scar treatment consistently identifies a hierarchy of approaches based on scar depth and subtype. For boxcar scars specifically, the evidence supports the following modalities:
- RF microneedling (Morpheus8): The strongest clinical evidence for boxcar scar improvement in the depth range most common in clinic populations. Delivers both mechanical microneedling stimulus and radiofrequency energy at calibrated depths, producing collagen remodeling through the full dermal thickness rather than just the surface layer.
- Subcision: Gold standard for deep boxcar scars with fibrous tethering. A blunt cannula inserted under the scar releases the fibrous band, allowing the scar floor to rise. Most effective when combined with RF microneedling in subsequent sessions to stimulate new collagen in the released space.
- Standard microneedling (SkinPen): Effective for shallow boxcar scars. Creates microchannels that stimulate collagen synthesis and can be combined with exosomes or PDRN for amplified regenerative response.
- Medium-depth chemical peels: Appropriate for shallow boxcar scars with significant surface texture component. Less effective for deeper scars where the issue is volumetric rather than textural.
- Combination protocols: For patients with mixed scar types or deep boxcar scars, a staged combination approach produces the best outcomes. Subcision first, followed by RF microneedling sessions, with SkinPen and exosomes for maintenance and surface refinement.
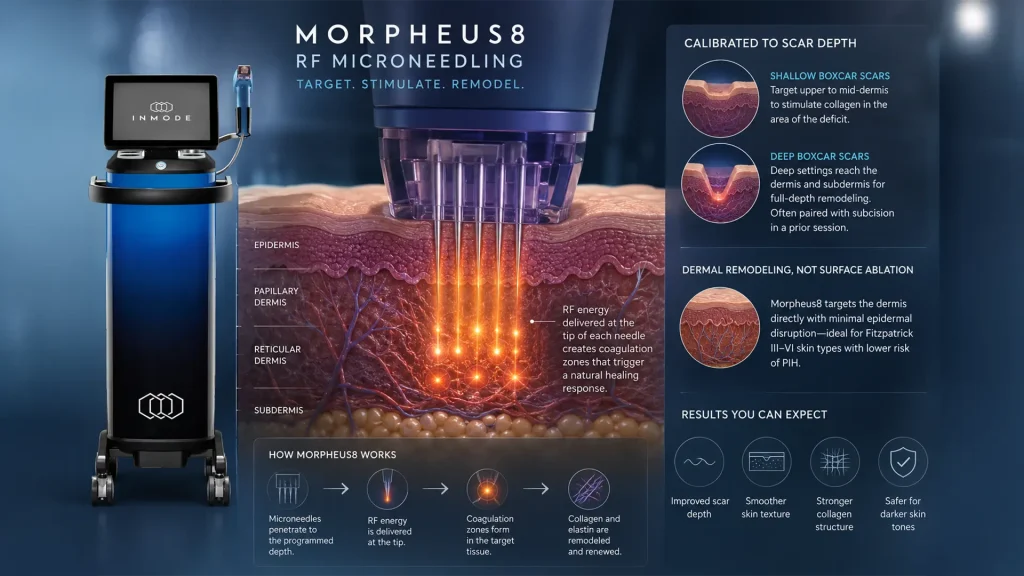
RF Microneedling and Boxcar Scars: What Morpheus8 Can Do
Morpheus8 is the RF microneedling device used at Perfect B for acne scar treatment. It combines a microneedling array with radiofrequency energy delivered at the tip of each needle at a programmable depth. This allows the APRN to target RF energy at the precise dermis layer most relevant to the scar being treated, rather than diffusing heat through the surface epidermis.
For boxcar scars, the depth and energy settings are calibrated to the scar’s depth profile. Shallow boxcar scars are addressed with settings that target the upper and mid-dermis where the collagen deficit is located. Deep boxcar scars require settings that reach deeper into the dermis and subdermis to stimulate remodeling in the full depth of the depression, and are often paired with subcision performed in a prior session.
The RF component of Morpheus8 produces coagulation zones at the needle tips that trigger a wound healing response from the body, producing new collagen and elastin in the treated area. Unlike laser resurfacing, which works by ablating the surface epithelium, Morpheus8 targets the dermis directly with minimal surface disruption, which is an important advantage for patients with Fitzpatrick III-VI skin types where surface ablation carries elevated post-inflammatory hyperpigmentation risk.
For a complete breakdown of Morpheus8 and RF microneedling at Perfect B, see our guide to RF microneedling for acne scars with Morpheus8. For patients whose boxcar scars are shallow and do not require RF depth, microneedling for acne scars with SkinPen provides a detailed overview of the standard protocol and what to expect from it.
Subcision for Boxcar Scars: Breaking the Fibrous Bands
Subcision is a minimally invasive procedure in which a blunt-tipped cannula is inserted through a small entry point adjacent to the scar and passed under the scar base to sever the fibrous bands connecting the scar floor to the deeper tissue. When the fibrous tether is cut, the scar floor is released and can rise toward the skin surface. The procedure also induces a localized inflammatory response that stimulates collagen production in the treated area, further supporting the volumetric recovery.
Subcision is indicated specifically for boxcar scars where physical examination confirms visible tethering. The classic sign is a scar that looks deeper when the skin is stretched laterally and shallower when compressed from below. If lateral stretch deepens the depression, the scar has a fibrous attachment that is being pulled tighter by the stretching skin. If the depression remains unchanged with lateral stretch, tethering is less likely and subcision may not add significant benefit over RF alone.
The sequence matters: subcision is generally performed first to release the tether, followed by RF microneedling sessions spaced four to six weeks apart to stimulate new collagen in the released space. Performing RF microneedling before subcision in a tethered scar stimulates collagen formation above the fibrous band but cannot address the underlying restriction that holds the scar floor down.
Skin Type Considerations: Fitzpatrick III-VI and Boxcar Scars in Doral
The majority of patients presenting for acne scar treatment at Perfect B in Doral have Fitzpatrick III-VI skin types. This population requires specific considerations that differ from the predominantly Fitzpatrick I-II populations most commonly used in published protocol studies.
The primary risk in higher Fitzpatrick skin types is post-inflammatory hyperpigmentation. Any treatment that triggers a significant inflammatory response can cause melanocytes to overproduce pigment, leaving darker patches in the treated area that can persist for months if not managed properly. For acne scar treatment, this means calibrating RF energy levels and depth settings to produce effective collagen remodeling without creating an inflammatory response large enough to trigger PIH in the surrounding skin.
Morpheus8 is well suited to this population because its depth-controlled RF delivery targets the dermis directly rather than heating the surface epidermis where melanocytes are concentrated. When settings are appropriate for the patient’s Fitzpatrick type, the surface disruption is minimal relative to the depth of collagen remodeling achieved. The APRN at Perfect B has extensive experience with Fitzpatrick III-VI patients and adjusts every protocol to the patient’s specific skin tone, baseline pigmentation status, and prior treatment history.
Frequently Asked Questions About Boxcar Scars
1. What do boxcar scars look like?
Boxcar scars are round or oval depressions in the skin with defined vertical walls and a flat base. They typically measure 1.5 to 4.0 mm across and are most common on the cheeks and temples. In raking light or direct flash photography, they show a sharp shadow at their edges. They look wider and more open than icepick scars and have more defined edges than rolling scars.
2. Are boxcar scars permanent?
Shallow boxcar scars can see significant improvement with appropriate clinical treatment and may become nearly invisible after a full series of sessions. Deep boxcar scars with fibrous tethering can be improved substantially but rarely achieve 100% correction. Most patients with deep boxcar scars can expect 50 to 70 percent improvement after a complete treatment series, which is clinically meaningful and often life-changing in terms of confidence and appearance, even if the scars are not entirely eliminated.
3. What is the best treatment for boxcar scars?
It depends on depth. Shallow boxcar scars respond well to RF microneedling with Morpheus8 or SkinPen microneedling with exosomes. Deep boxcar scars with fibrous tethering benefit most from subcision followed by RF microneedling sessions. The right treatment is determined at an APRN intake where scar depth and skin type are assessed before any protocol is selected.
4. Can microneedling fix boxcar scars?
Standard microneedling is effective for shallow boxcar scars. For deep boxcar scars with fibrous tethering, standard microneedling alone typically produces incomplete results because it cannot address the fibrous band holding the scar floor down. RF microneedling reaches deeper layers and is more effective for moderate-depth boxcar scars, but deep scars with significant tethering still benefit from subcision before surface treatment.
5. Does subcision work for boxcar scars?
Yes, specifically for boxcar scars where physical examination confirms fibrous tethering. Subcision releases the fibrous band connecting the scar base to the deeper tissue, allowing the scar floor to rise. It is most effective when combined with RF microneedling sessions after the release to stimulate collagen in the newly freed space. It is not indicated for all boxcar scars, only those with confirmed tethering.
6. What is the difference between boxcar and icepick scars?
Icepick scars are narrow and deep with a V-shaped channel. Boxcar scars are wide with vertical walls and a flat base. They require completely different treatments: TCA CROSS is used for icepick scars and is not appropriate for boxcar scars. Microneedling and RF are primarily used for boxcar scars. Many patients have both types simultaneously, which requires a combined protocol designed for each.
7. How many sessions does it take to treat boxcar scars?
Most patients complete three to five RF microneedling sessions spaced four to six weeks apart for shallow to moderate boxcar scars. Deep boxcar scars with subcision may require more sessions and a longer overall timeline. Significant visible improvement is typically apparent after the second or third session, with results continuing to develop for several weeks after the final session as new collagen matures.
8. Is TCA CROSS used for boxcar scars?
No. TCA CROSS is a technique designed specifically for icepick scars, not boxcar scars. It involves applying high-concentration TCA to the narrow base of an icepick channel to trigger focal collagen remodeling at depth. Boxcar scars have a wide base that does not concentrate the acid the way an icepick channel does, making TCA CROSS ineffective for boxcar anatomy and potentially harmful. At Perfect B, TCA CROSS is used only for confirmed icepick scars.
Closing: Boxcar Scars Require the Right Assessment Before the Right Treatment
Boxcar scars are not all the same. A shallow boxcar scar on a Fitzpatrick III patient who has never had clinical treatment is a very different clinical problem from a deep, tethered boxcar scar on a Fitzpatrick V patient who has had multiple prior sessions elsewhere without meaningful improvement. The treatment that produces the best outcome in the first case is not the same treatment that addresses the second.
At Perfect B in Doral, the intake consultation is where treatment decisions are actually made, not at the treatment chair. The APRN classifies scar type, assesses depth and tethering, evaluates skin tone and prior treatment history, and builds a protocol that sequences the right interventions in the right order for the specific patient.
📍 Perfect B | 8200 NW 41st St, Suite 100, Doral, FL 33166
📞 (786) 502-2260


