
Perfect B, Doral Fl. | 06.19.26 | 12 min read.
This article is for general educational purposes and does not replace a medical evaluation. Scar revision with polynucleotide therapy should only be considered after an in person clinical assessment by a licensed provider, and the information below does not constitute a diagnosis, prescription, or treatment plan.
Key Takeaways
- PDRN for surgical scars is a regenerative layer, not a replacement for standard scar care. Silicone sheeting, sun protection, and incision support remain the baseline; PDRN injections add fibroblast and vascular remodeling to that base.
- Surgical and trauma scars mature over 12 to 18 months according to Memorial Sloan Kettering patient guidance, and PDRN can be considered at different points across that window depending on the healing phase.
- Early postoperative PDRN can reduce hypertrophic scar risk. A 2023 randomized clinical trial of PDRN injections after thyroidectomy reported significantly lower vascularity and lower modified Vancouver Scar Scale scores at three months.
- Established scars also respond. For atrophic scar treatment of C-section, abdominoplasty, or laparoscopy scars, and for hypertrophic or revision scars, PDRN can be layered with microneedling, subcision, or laser as the clinical picture requires.
- The clinical question is timing and stacking, not whether the molecule works. What changes between patients is the healing phase, scar morphology, skin tone, and what other modalities the scar has already seen.
Why Surgical and Trauma Scars Need More Than Silicone and Sunscreen
For most patients with a new surgical wound or a post-trauma scar, surgical scar treatment advice has not changed in fifteen years: silicone sheeting or gel for several months, daily sun protection, and gentle massage once the incision is fully closed. That trio is real and worth doing. It is also incomplete from a pdrn scar revision perspective. Silicone helps the surface; it does not change what the dermis is doing underneath. The actual cellular work of scar formation, the collagen orientation, the small blood vessel density, the elasticity of the new tissue, happens below the surface, and it follows a timeline that runs well beyond the few months that most home protocols cover.
Patient guidance from Memorial Sloan Kettering’s clinician resource on caring for surgical scars after skin surgery states that a scar continues to heal for 12 to 18 months after surgery. That window is the entire reason a regenerative layer like a pdrn scar revision protocol exists in modern aesthetic practice. The question is not whether the standard of care works; it is what you can add to it during that 18 month window to give the scar a better final outcome. This guide is about that addition: pdrn for surgical scars, how a polynucleotide protocol fits inside the standard of care, who it serves, and what a medical clinic in Doral, FL does with it on real patients.

What PDRN (Polynucleotides) Actually Is, in Plain English
Polydeoxyribonucleotide, abbreviated PDRN, is a fragment of purified DNA derived from controlled salmon trout milt and standardized for medical use. It is not a filler; it does not change facial volume. It is not a peptide; it does not signal hormones. It is a piece of DNA that, when injected into the dermis, binds the A2A adenosine receptor on fibroblasts and on local vasculature. The downstream effect is two clinical changes that matter in scar tissue: fibroblast activity goes up, and inflammatory and vascular tone goes down. Translated into outcomes, that is a scar that lays down better organized collagen and that calms the redness, raised tone, and itch that classically signal a scar maturing the wrong way.
If you want the full mechanism in one place, our deep dive on what PDRN is, how polynucleotides differ from dermal fillers, and what the molecule actually does in the skin walks through the cellular pathway and the FDA category nuance. For the rest of this article, the practical short version is enough: PDRN is the regenerative layer you can add on top of silicone, sun protection, and any device-based scar work the patient has already had.
How PDRN Behaves Differently in Scar Tissue vs Normal Skin
In healthy skin, PDRN is a slow regenerative tune up: better hydration retention, slightly better elasticity, modest brightening over a few sessions. In scar tissue the same molecule is doing something else, because scar tissue is built on a disorganized collagen scaffold with abnormal capillary density. Fibroblasts inside a hypertrophic or raised scar are still active and still depositing collagen long after they should have stopped. PDRN modulates that. It supports fibroblasts in a remodeling direction rather than a runaway proliferation direction. It also reduces the small vessel network feeding the scar, which is what most patients perceive as redness or that pinkish raised edge that does not fade with time alone.
This is why scar protocols look different from cosmetic ones. The visits target the scar itself with a small needle along the edges and through the scar bed, the cadence is set by where the scar is in its maturation curve, and the endpoint is a flatter, less vascular, better textured final scar, not a brighter face.
Which Surgical and Trauma Scars Respond to PDRN at Our Doral Clinic
The label “surgical scar” hides a wide range of clinical realities, so the assessment matters more than the category. The scars Perfect B sees most often in this protocol fall into a few buckets:
- C-section scars and abdominoplasty scars. Long, low-tension linear scars that frequently develop a small atrophic depression and benefit from atrophic scar treatment, a darker color, or in some Fitzpatrick types a raised hypertrophic band. Atrophic scar treatment in this category supports remodeling, with microneedling or subcision added when there is structural depression.
- Thyroidectomy and neck surgery scars. High visibility, high cosmetic stakes, and a known risk for hypertrophic transformation. The Kim 2023 trial cited below specifically studied PDRN in this population.
- Breast surgery scars. Augmentation, reduction, and lift incisions. Variable morphology by patient, and PDRN can be considered once incisions are stable.
- Laparoscopic port scars and mole excision scars. Small but often raised or darkened. Quick to remap.
- Trauma scars and ER closure scars. Lacerations from accidents, dog bites, glass injuries, kitchen and workshop wounds. Often closed by someone who is not a plastic surgeon. These are the scars patients most commonly want revised one to three years later.
- Revision-of-revision scars. Scars that already had a surgical revision and need a regenerative push to get the last 20 to 30 percent of improvement.
The mapping logic is similar to what we use in the stretch mark protocol. For patients whose scar runs through tissue that has stretched, our companion guide on how PDRN supports dermal remodeling in stretch marks and how the protocol changes based on whether striae are red or white covers a closely related decision framework.

When to Start PDRN After Surgery or Trauma: The Healing Phase Question
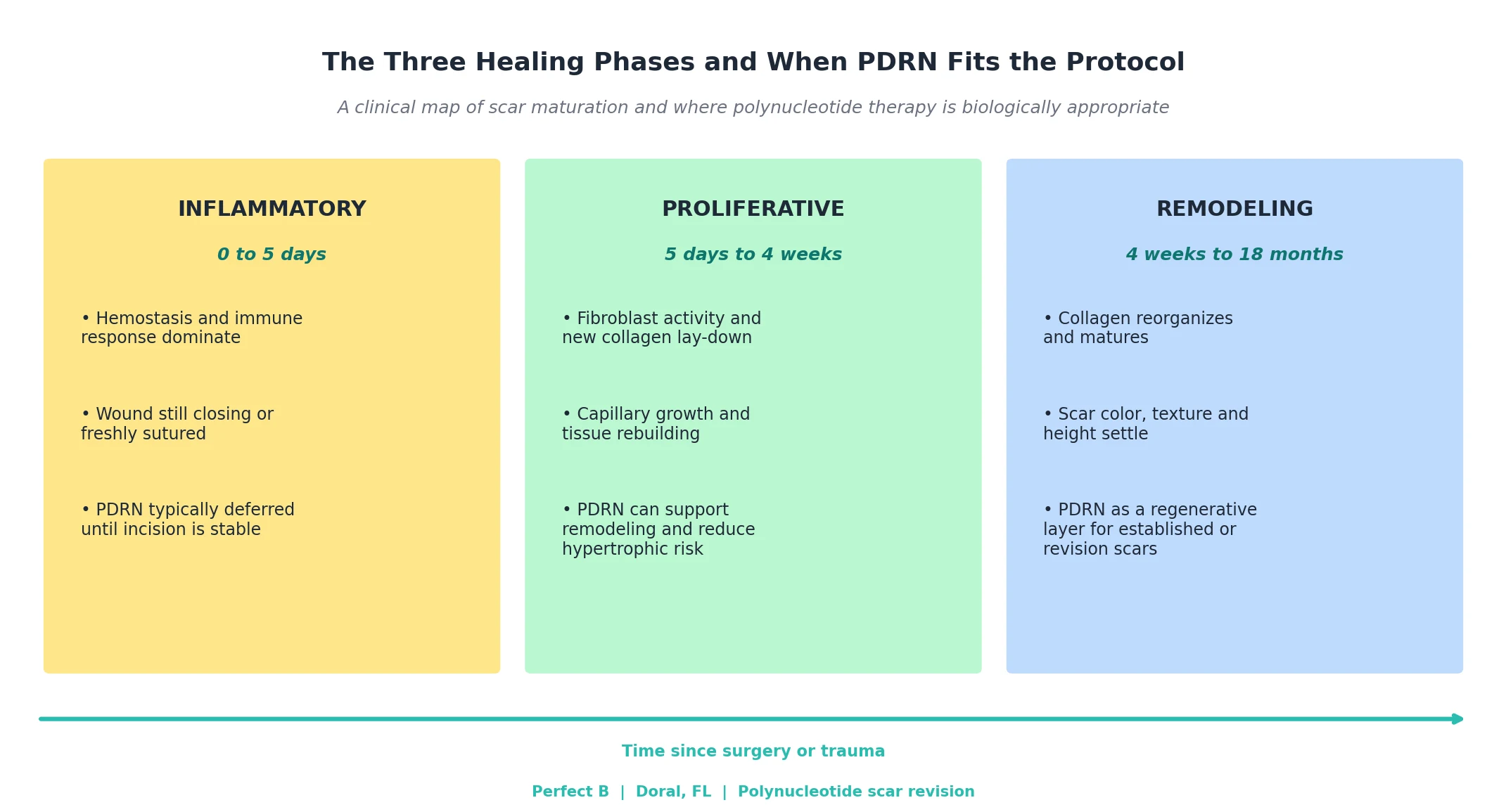
Scars heal in three overlapping phases, and where the scar is in those phases changes what is biologically appropriate. The inflammatory phase covers roughly the first five days while the wound is closing and the immune response dominates. The proliferative phase runs from about day five through the first month, while fibroblasts lay down new collagen and small vessels reorganize. The remodeling phase begins around week four and continues for the rest of the 12 to 18 month scar maturation window, while collagen reorients and the scar settles in color, height, and texture.
The most studied use of pdrn for surgical scars is in the early postoperative window. A 2023 randomized controlled trial in Aesthetic Plastic Surgery on early postoperative polydeoxyribonucleotide injections after thyroidectomy reported lower modified Vancouver Scar Scale scores and a significantly lower vascularity subscore at three months in the patients who received PDRN, leading the authors to conclude that early postoperative PDRN injection is an effective and safe treatment to prevent hypertrophic scars. That is the proliferative-phase use case for pdrn for surgical scars. For established scars in the remodeling phase, the same molecule is used in a different cadence and often stacked with subcision, microneedling, or laser to address structural depression or surface texture that PDRN alone is not designed to correct.
How a PDRN Scar Revision Visit Actually Works at Perfect B in Doral
A first visit when patients search scar revision near me and book at our Doral, FL clinic is built around the scar, not around a generic facial protocol. The provider takes a focused surgical and trauma history, including how long ago the wound occurred, who closed it, whether the patient has any keloid history, and whether the scar has already been treated with silicone, steroid injections, laser, or surgical revision. The scar is then mapped: length, depth, color, raised versus depressed segments, vascularity, and the relationship to nearby anatomy that limits how the scar contracts and pulls.
Only after that workup is a protocol set. PDRN may be the lead modality, or it may be the regenerative layer added to subcision, RF microneedling, or a fractional resurfacing laser depending on what the scar needs. The visit itself involves a topical anesthetic, a small-gauge needle, and a series of small injections placed along the scar bed and edges. Patients leave with written aftercare and a written plan for the next visit. There are no specific doses or session counts in this article because the right number for a given scar depends on the scar in front of the provider, not on a number that reads well in a blog post.
PDRN vs Steroid Injections, Lasers, Subcision, and Silicone: How They Stack
None of the available scar modalities does everything, and pdrn scar revision is no exception. They each solve a different part of the problem, and a real protocol is usually a stack rather than a single tool.
- Silicone sheeting or gel: a base-of-care surface modality that hydrates the stratum corneum and modulates fibroblast signaling. Cheap, evidence based, and worth the months of compliance for any new surgical scar.
- Sun protection: not optional. Sun exposure in the first year drives pigment change in scars, especially in Fitzpatrick III to VI skin, which is the majority of our South Florida patient population.
- Intralesional steroid: the standard injectable for raised hypertrophic and keloid scars. Powerful but blunt, with thinning and pigment loss as real downsides. PDRN is not a steroid replacement; the two address different mechanisms.
- Subcision: the structural release of tethered scar tissue, used for depressed scars where fibrous bands pull the surface down. PDRN layered after subcision supports the remodeling phase.
- RF microneedling and fractional laser: resurfacing modalities that drive collagen remodeling through controlled injury. Effective for texture; often paired with PDRN as the regenerative layer for the recovery window.
- PDRN: the regenerative layer that supports fibroblast remodeling and reduces vascularity. Effective on its own for many scars, and stack-ready with most of the above.
The surgical scar treatment protocol your scar needs depends on the morphology and where it is in maturation. That is the conversation a real consultation answers, and it is the reason a clinic plan beats a single-product purchase.
Is PDRN Safe for Post-Surgical and Trauma Scars?
PDRN as a clinical class has a strong safety profile when administered by a licensed clinician using product from a regulated source. Side effects are typically limited to mild injection-site reactions, transient redness, small bruising, and short-lived tenderness. The product is salmon-derived and purified, and patients with documented severe salmon or fish allergy should disclose that history; in those cases PDRN is generally not used. Patients with active infection in the scar area, untreated dermatologic disease at the site, pregnancy, breastfeeding, or active systemic illness should defer until cleared.
For a full review of the safety profile across the dermatologic literature, including the regulatory framework and the documented side-effect distribution, our companion piece on whether PDRN is safe, what the documented side effects are, and who should not receive it covers the topic in depth. The short version is that safety in scar revision is overwhelmingly a function of who is injecting and what is in the vial, not of the molecule itself.

What a Scar Revision Plan Looks Like at Perfect B in Doral, FL
For most patients the plan opens with a 30 minute mapping consultation. We document the scar with measured photographs, classify it, review the surgical or trauma history, and set realistic expectations for what PDRN can and cannot do given the morphology in front of us. If PDRN is appropriate, we schedule the first visit at the right point in the healing curve. If the scar needs structural work first, we coordinate subcision, RF microneedling, or fractional resurfacing into the plan and slot PDRN as the regenerative layer in the recovery window.
Throughout the plan, patients keep doing the basics that work: silicone sheeting or gel for new scars in the first months, sun protection daily, and gentle massage once the incision is fully closed. The point of a scar revision near me clinic visit is to add a layer the home protocol cannot reach, not to replace what already works.
Frequently Asked Questions
1. How soon after surgery can I start PDRN for my scar?
Timing depends on what the wound is doing. For sutured incisions, providers typically wait until sutures are out and the wound is closed and stable, then evaluate whether the proliferative phase is the right window to begin. For trauma scars closed in an ER weeks or months ago, the answer is different and usually faster to plan. A mapping visit gives the right answer for your specific scar.
2. Does PDRN work on C-section scars from years ago?
Yes, for many patients. Older C-section scars in the remodeling phase respond to PDRN, particularly when there is a small depression, color change, or raised band along part of the scar. For atrophic scar treatment of scars with significant tethering or contour irregularity, subcision is usually added to address the structural component, with PDRN layered as the regenerative support.
3. Is PDRN safe if my skin is keloid prone?
Keloid history changes the protocol. PDRN does not directly suppress runaway collagen the way intralesional steroid does, so for active keloids the lead modality is usually steroid and the PDRN role is supportive once the keloid is under control. The decision belongs to a clinical evaluation, not to a generic recommendation.
4. Can I combine PDRN with my laser or microneedling sessions?
That is one of the most common stack patterns in modern scar revision. PDRN supports the recovery and remodeling phase after a device-based treatment, which is why many protocols schedule PDRN injections shortly after laser or RF microneedling sessions rather than as standalone visits.
5. What does the downtime look like after a PDRN scar session?
Most patients see mild redness at injection points, small bruising in some areas, and tenderness along the scar for one to two days. There is no peeling, no recovery from a resurfacing window, and most patients return to work the same day or the next day. Sun protection on the scar is mandatory throughout the protocol.
6. Is pdrn for surgical scars covered by insurance?
Scar revision with PDRN is generally treated as an aesthetic procedure and is not covered by medical insurance. Perfect B works with patients on financing through Cherry, Klarna, Afterpay, and CareCredit so the program can be paid over time. We do not quote a single number on the blog because the right plan depends on the scar; pricing is set during the consultation.
7. Can I do PDRN if I am pregnant or breastfeeding?
No. Pregnancy and breastfeeding are standard deferral periods for elective injectable aesthetic procedures, including PDRN. Patients with a recent C-section who want to address the scar should wait until they are no longer pregnant or nursing and have been cleared by their obstetric team.
8. How long until I see a change in the scar?
PDRN is not an overnight result. For patients who searched scar revision near me and started a clinic plan, most begin to notice change in scar redness, softness, and texture across the first six to twelve weeks, with continuing improvement through the maturation window that MSKCC describes as 12 to 18 months. The goal is a better final scar at the end of that window, not an immediate transformation.
Closing: The Clinic Bottom Line on PDRN for Surgical and Trauma Scars
Surgical scars and trauma scars finish maturing somewhere between 12 and 18 months after the injury, and what you add inside that window changes the final outcome. The standard of care for surgical scar treatment, silicone and sun protection, is real and worth doing, but it is a surface layer for a problem that lives in the dermis. PDRN, used by a licensed clinician at the right phase of healing and stacked with the right structural or resurfacing modality where needed, is the regenerative layer that turns standard of care into a real protocol.
At Perfect B in Doral, FL, the alternative to a generic scar gel for surgical scar treatment is a clinical plan that puts pdrn for surgical scars inside a documented protocol: a mapping visit, a written scar revision near me protocol tailored to the morphology of your scar, a transparent decision on whether PDRN should lead or layer, and a real follow-up schedule across the maturation window. If you are weighing the home aisle against a clinical scar revision plan, the comparison is not close.
- 📍 Perfect B | 3905 NW 107th Ave, Suite 104, Doral FL 33178
- 📞 Call or message us at (786) 502-2260
- 💳 Buy Now Pay Later: Cherry, Klarna, Afterpay, CareCredit


