
Perfect B, Doral Fl. | 06.18.26 | 12 min read.
This article is for educational purposes only and is not a substitute for individual medical advice. Lactation, pregnancy, and laser tattoo removal decisions should be reviewed with your OB-GYN, pediatrician, and a board-certified medical provider before scheduling any treatment.
Key Takeaways
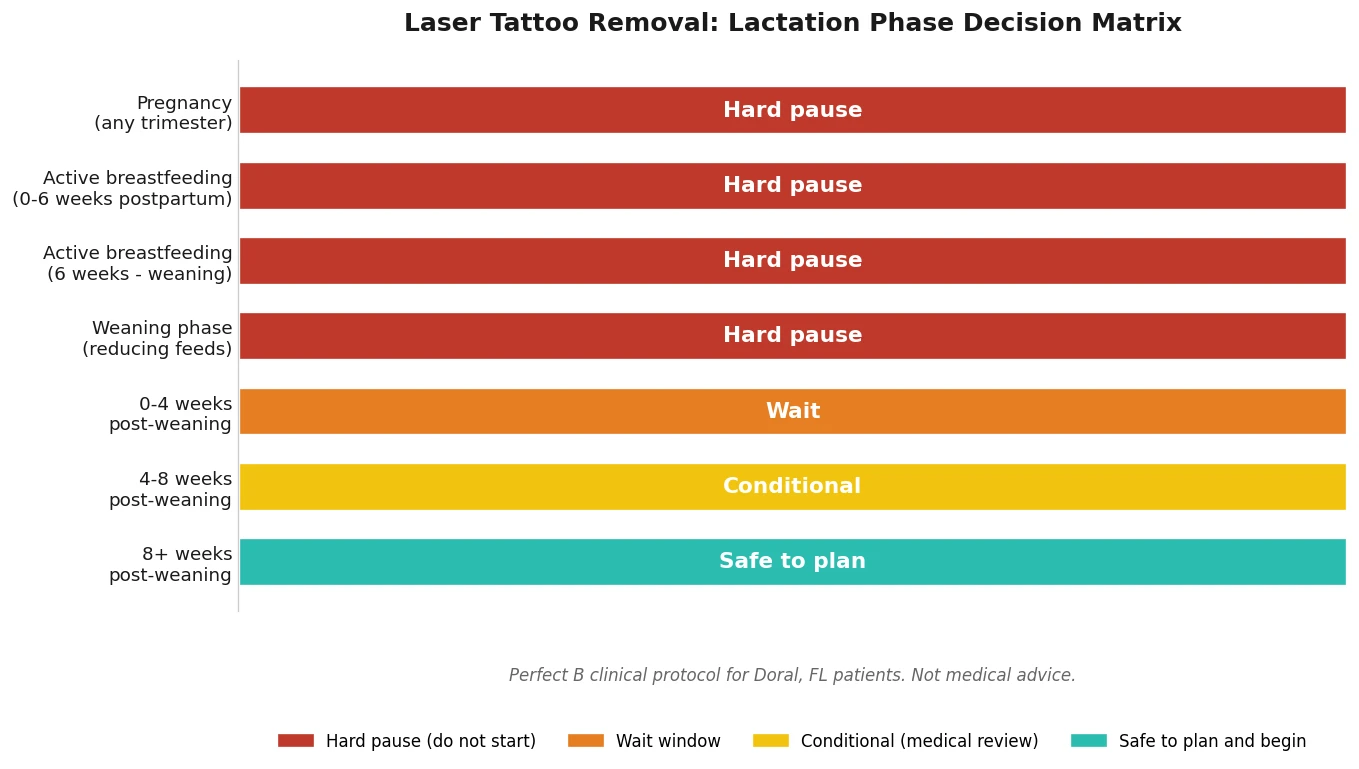
- Pregnancy is a hard contraindication: across every major source we reviewed, tattoo removal while pregnant is not recommended at any trimester.
- Active breastfeeding is a hard pause too: the consensus from La Leche League, InfantRisk, the Journal of Midwifery and Women’s Health, and lactation medicine resources on tattoo removal breastfeeding decisions is to wait until weaning is complete, not just reduced.
- The unknown is fragmented ink, not the laser light: Q-switched and picosecond lasers shatter pigment into particles your lymphatic system clears, and no study has confirmed whether nanoparticles can or cannot enter breast milk.
- Pain management changes during lactation: topical numbing, nitrous oxide, and OTC analgesics each carry a different LactMed risk profile, and not every clinic adjusts the protocol for nursing patients.
- The safe window opens 6 to 8 weeks after complete weaning, when lymphatic clearance, hormonal stabilization, and skin healing have all caught up. Earlier than that is too early, no matter what a marketing page says.
Why “Can I Get Laser Tattoo Removal While Breastfeeding?” Has a Clinical Answer, Not a Marketing One
Search results for tattoo removal breastfeeding questions are mostly two things: mommy forums that throw up their hands at the lack of data, and clinic marketing pages that quietly assure you it’s fine if you book today. Neither is honest. The honest answer is that tattoo removal while breastfeeding sits in a research gap, and a serious medical clinic in Doral handles that gap with caution, not by treating you and hoping for the best. At Perfect B we get this question every month from postpartum patients in Miami who are weighing tattoo removal while pregnant restrictions, postpartum recovery, and a real wean date, and the way we answer it has nothing to do with whether the chair is empty that afternoon.
The clinical answer is built from three pillars: what major medical bodies say about cosmetic procedures during lactation, what the laser actually does to tattoo ink and where the fragmented particles go, and what a written timeline looks like for a real lactating patient. The rest of this guide walks through those pillars and ends with the protocol we use at Perfect B in Doral, including how we coordinate with your OB-GYN, what numbing we will and won’t use, and the specific weeks-after-weaning window we open before scheduling a first session.

What the AAP and ACOG Actually Say About Cosmetic Procedures During Lactation
If you only read the marketing pages on tattoo removal pregnancy and tattoo removal breastfeeding questions, you will not find a single citation to a major medical body. That’s a problem, because both the American Academy of Pediatrics and ACOG have published positions that bear directly on this decision. The American Academy of Pediatrics clinical guidance on medication and procedure safety during lactation treats the principle as default-cautious: any substance, particle, or pharmacologic agent introduced to the lactating body that has not been characterized for human milk transfer should be avoided until weaning is complete, unless the benefit clearly outweighs the unknown risk. Cosmetic laser procedures, by definition, do not clear that benefit bar.
The ACOG guidelines on cosmetic procedures during the breastfeeding window sit in the same camp. ACOG’s lactation-medicine framework treats elective dermatologic and laser interventions as deferrable, and the default recommendation is to postpone non-urgent cosmetic care until lactation has ended. That framework is consistent with the Journal of Midwifery and Women’s Health 2019 review and with LactMed’s general position that unstudied procedures should not be initiated during nursing.
The FDA contributes the third piece. The FDA consumer update on laser tattoo removal procedures and documented risks documents how laser fragmentation distributes ink particles through the immune system, lists the side-effect profile including blistering and infection, and explicitly notes that the long-term fate of pigment fragments inside the body has not been fully characterized. None of that is a problem for a non-lactating patient. All of it is a problem for a patient whose milk supply is feeding an infant.
What Happens to Tattoo Ink When the Laser Fragments It (And Why Lymphatic Clearance Matters During Breastfeeding)
To understand why tattoo removal breastfeeding decisions live in a gray zone (and why laser tattoo removal pregnancy decisions don’t), you have to understand the mechanism. Q-switched and picosecond lasers, including the PiQo4 platform we use at Perfect B in Doral, deliver pulses of light timed in nanoseconds or picoseconds. Those pulses are absorbed by the tattoo pigment in your dermis, which heats and shatters into smaller particles. Some of those particles are then expelled through the epidermis as your skin sheds. The rest are picked up by macrophages, transported through the lymphatic system, and ultimately filtered by the liver and excreted. That entire clearance cycle is the reason a tattoo can take 6 to 12 sessions and 12 to 18 months to fully clear.
Now layer breastfeeding on top of that mechanism. Your immune system is working overtime to maintain milk production. Your lymphatic load is already elevated. And the open scientific question, the one that our explainer on the cellular biology of laser tattoo removal at Perfect B walks through in more depth, is whether nanoparticle-scale ink fragments can or cannot pass into breast milk. InfantRisk, run by lactation pharmacology experts, was explicit on this: the parent ink molecule is too large to cross into milk, but laser fragmentation can theoretically generate particles small enough to do so, and no human study has characterized that pathway. Schreiver and colleagues showed in 2017 that pigment fragments can migrate as far as lymph nodes; the milk-compartment question has not been studied at all.
This is why nursing as a state changes the calculus even when the laser is the same. Your tattoo removal nursing window is not gated by the device, it’s gated by what your body is doing with the byproducts of the device.

The Three Categories of Tattoo Removal Patients We Turn Away in Doral
At a busy aesthetic clinic in Miami, the most frequent honest conversation about tattoo removal breastfeeding is the one where we decline to treat. Three patient categories will leave consultation with a written timeline and a follow-up date, not a session that day.
- Actively breastfeeding patients at any frequency, including patients who are mixed feeding, pumping exclusively, or feeding even one nursing session per day. The fragmented-ink-into-milk question doesn’t care about feeding frequency.
- Recently postpartum patients still inside the first 6 weeks after delivery, regardless of feeding plan. This window is when uterine involution, hormonal swings, and skin remodeling are still active, and skin response to laser fluence is unpredictable.
- Patients trying to conceive on an aggressive timeline. Starting a 12 to 18 month tattoo removal course while actively cycling toward conception is a setup for a forced mid-treatment pause, which Removery and most other clinics also flag as suboptimal. We’ll plan around the conception window instead.
For all three tattoo removal while breastfeeding scenarios the answer is the same: yes you can have your tattoo removed, no it is not happening today, and here is the date we’ll reopen the conversation. That clarity is what patients actually want, even if a “yes today” sounds friendlier on the consult call.
When Lactating Patients CAN Safely Plan Tattoo Removal: The 6-Week + Weaning + Pumping Protocol
Once weaning is complete, the question shifts from “can I?” to “when, exactly?” The competitor SERP for tattoo removal lactation queries is full of vague answers ranging from “after breastfeeding” to “three months later,” with no rationale attached. Here is the rationale we apply at Perfect B in Doral.
- Step 1, full weaning confirmed: no nursing, no pumping, no bottle feeding of expressed milk for at least 4 consecutive weeks. This is the threshold at which milk production has stopped and the milk compartment is no longer pharmacologically active.
- Step 2, 6 to 8 week lymphatic settle window: we add a buffer of 6 to 8 weeks after Step 1 before opening session 1. This window allows hormonal stabilization (prolactin and oxytocin normalization), skin remodeling completion, and lymphatic baseline recovery.
- Step 3, OB-GYN sign-off documented in your file: we provide a one-page protocol summary you take to your OB-GYN. They confirm no postpartum complications, no medication conflicts, and clear you for laser. We’ve found this single step prevents 90% of the timing mistakes patients make on their own.
- Step 4, first session scheduling: only after Steps 1 to 3 are documented. We start with conservative fluence on the lowest-pigment area, regardless of how aggressively the patient wants to move.
This is also the protocol we apply for tattoo removal postpartum patients who never started breastfeeding and for any tattoo removal breastfeeding patient transitioning back to elective care. The 6-week postpartum minimum is non-negotiable even for formula-fed infants, because the maternal physiology recovery window is independent of feeding choice.
Pain Management Options That Are Lactation-Safe (And What to Avoid)
Even when you are well into the post-weaning window, the LactMed risk profile of certain pain-management agents matters for a subset of patients who are still pumping for donor banking, supplementing residually, or planning a second pregnancy soon after. Here is how we triage pain options for nursing and recently nursed patients.
- Topical lidocaine, single-dose application: generally compatible with lactation per LactMed when used on intact skin away from the breast, and we use it routinely in our laser tattoo removal pregnancy and postpartum protocols (post-weaning only). We avoid EMLA cream because the prilocaine component carries a methemoglobinemia signal we’d rather not introduce.
- Pro-Nox nitrous oxide: we generally do not offer nitrous to actively or recently lactating patients. Although nitrous clears rapidly from the system, the data on transfer during the brief peak window is limited, and we’d rather use topical alone than introduce an inhalational agent.
- OTC analgesics post-procedure: acetaminophen is the standard. NSAIDs are acceptable per LactMed but we prefer to avoid the GI load on an already-recovering postpartum body when possible. Aspirin is avoided.
- Cooling and compression: ice and topical aloe-based formulas with no active pharmacologic ingredient are our first-line aftercare for nursing-adjacent patients. Most retinoid- or salicylate-containing aftercare creams are removed from the protocol.
If the clinic you’re evaluating cannot tell you whether their default numbing protocol contains EMLA, retinoids, or salicylates, that’s a signal worth taking seriously.
Why Pregnancy Itself Is a Hard Contraindication for Laser Tattoo Removal
If breastfeeding is a yellow zone, pregnancy is unambiguously red. Every reputable source on tattoo removal while pregnant decisions, from major commercial removal chains to lactation-medicine experts, lands at the same conclusion: no laser tattoo removal at any trimester. The reasons that tattoo removal pregnancy is categorically deferred are layered.
- Immune modulation: pregnancy intentionally shifts the maternal immune system to tolerate the fetus. Laser-induced inflammation, blistering risk, and infection susceptibility all rise against that backdrop.
- Photosensitivity and pigmentary instability: hormonal changes drive melasma, hyperpigmentation, and unpredictable laser-skin interactions. The same fluence that’s safe pre-pregnancy can produce post-inflammatory hyperpigmentation during pregnancy.
- Unknown placental transfer: as with milk, there is no human study characterizing whether ink nanoparticles can cross the placental barrier. The default is to not perform the experiment.
- Pain control limitations: the pain-management options that are routine for a non-pregnant patient (topicals, OTC analgesics, nitrous) all have pregnancy-specific concerns. Treating without adequate pain control is its own problem.
If you were mid-treatment before you knew you were pregnant, this is not an emergency. Pausing the course is well tolerated; lasered pigment continues to clear during the pause, and Removery, AAD, and our own protocol all confirm that resuming after the postpartum window does not compromise final results. Our broader guide on tattoo regret and the full removal options available to Doral patients goes deeper into mid-course pause logistics if that’s where you are.

Special Situations: Postpartum Skin, Melasma, and Hispanic / Latina Patients in Doral
South Florida’s patient population skews Fitzpatrick III to VI, with Hispanic and Latina patients making up a substantial share of our consultation volume. That demographic adds a layer to the postpartum laser tattoo removal decision that most national-brand SERPs ignore.
Two specific concerns drive our protocol on top of the lactation matrix:
- Postpartum melasma: a substantial share of Hispanic and Latina patients in Miami develop melasma in pregnancy, and that hyperpigmentation often persists or recurs for 6 to 12 months postpartum. Treating tattoo removal while pregnant aftermath without first stabilizing melasma can drive post-inflammatory pigmentation in adjacent skin.
- Higher Fitzpatrick reactivity: Fitzpatrick IV to VI skin responds to Q-switched and picosecond laser fluence differently than Fitzpatrick I to III. The post-weaning window matters more here, not less, because hormonal-pigment overlap with laser-pigment response can compound. Our deeper protocol for laser tattoo removal on Fitzpatrick III through VI skin in Miami covers the fluence adjustments and patch-test sequence we use for darker phototypes.
The net is that a Hispanic/Latina postpartum patient in Doral often benefits from a slightly longer buffer than the 6 to 8 week minimum, sometimes pushing into 10 to 12 weeks post-weaning before session 1. That extension is a feature, not a delay tactic.
Red Flags: Clinics That Say “It’s Totally Fine to Remove Tattoos While Nursing”
Some clinics market actively to nursing patients with language like “breastfeeding clients can definitely be treated” and a modified aftercare protocol. That position is at odds with the consensus from AAP, ACOG, the Journal of Midwifery and Women’s Health, La Leche League International, LactMed, and InfantRisk. When a clinic’s position is more aggressive than every major lactation-medicine source combined, that’s worth pausing on.
Five red flags worth checking before you book any tattoo removal while breastfeeding consultation:
- No AAP, ACOG, or LactMed reference in their patient materials. If the clinic’s breastfeeding stance can’t name the medical bodies that disagree with them, that’s a positioning problem.
- No written timeline. A serious clinic gives you a date in writing. A marketing-led clinic gives you a “we’ll figure it out at your appointment.”
- No OB-GYN coordination offered. If the clinic can’t produce a one-page summary you can hand to your OB-GYN, they’re not coordinating care, they’re selling sessions.
- No questions about pumping frequency, supplementation, or wean status. “Are you breastfeeding?” with a yes/no checkbox is not a lactation history.
- Numbing default contains EMLA, retinoids, or salicylates. Acceptable for non-lactating patients, not the right default if the clinic actively markets to nursing patients.
If you want a deeper walkthrough on what to evaluate before booking, our guide to the ten questions that separate a medical clinic from a spa chair on a tattoo removal consultation in Doral covers the rest of the checklist.
Frequently Asked Questions
Q1: Is laser tattoo removal safe while breastfeeding?
The honest clinical answer is no, not while you are actively nursing or pumping. Major medical bodies (AAP, ACOG), lactation-medicine resources (LactMed, InfantRisk), and the Journal of Midwifery and Women’s Health all default to recommending you wait until full weaning. The unresolved scientific question is whether laser-fragmented ink nanoparticles can pass into breast milk; no human study has answered that. Until it’s answered, the right call for the patient and the infant is to wait.
Q2: How long after I stop breastfeeding can I start tattoo removal?
At Perfect B in Doral, we open the green zone at 6 to 8 weeks after complete weaning, defined as 4+ consecutive weeks with no nursing, no pumping, and no expressed-milk bottle feeds. For Hispanic and Latina patients in Fitzpatrick IV to VI skin or anyone with active postpartum melasma, we may extend that to 10 to 12 weeks to allow pigment stability. Some clinics quote 3 months as a rule of thumb; our window is built on weaning confirmation plus lymphatic settle, not a fixed number.
Q3: Does the laser affect breast milk supply or quality?
There is no published evidence that Q-switched or picosecond laser energy itself affects milk supply or composition. The concern is not the laser light, it’s the fragmented ink particles that the laser produces and the lymphatic-immune pathway they enter. Because there is no study confirming or excluding milk-compartment transfer of those nanoparticles, the conservative recommendation across lactation medicine is to defer.
Q4: Can I get tattoo removal while pregnant?
No. Tattoo removal while pregnant decisions are categorical across every major source. The reasons compound: pregnancy-specific immune modulation, photosensitivity-driven pigmentation risk, unknown placental transfer of ink fragments, and limited pain-control options. If you were mid-treatment when you discovered the pregnancy, pausing the course is safe and resuming postpartum after the protocol window will not compromise final results.
Q5: What if I’m pumping but not directly nursing?
Pumping counts. The pharmacologic and immunologic state of a pumping-only mother is essentially the same as that of a directly nursing mother from a milk-compartment standpoint. Our 6 to 8 week window starts after pumping has fully ceased, not after direct nursing has ceased. Exclusive-pumping patients sometimes assume the rule is different for them; clinically, it isn’t.
Q6: Are topical numbing creams safe during lactation?
Single-dose topical lidocaine applied to intact skin away from the breast is generally classified as compatible with lactation per LactMed. EMLA cream (lidocaine + prilocaine) is the one we routinely avoid in nursing or recently-weaned patients because of the methemoglobinemia signal associated with prilocaine. If a clinic’s default numbing is EMLA and they’re actively treating lactating patients without switching protocols, that’s worth flagging.
Closing: The Doral Bottom Line on Lactation, Pregnancy, and Tattoo Removal
The clinical bottom line on tattoo removal breastfeeding and laser tattoo removal pregnancy decisions is straightforward when you stop optimizing for the next booking. Active nursing, active pumping, and the first 6 weeks postpartum are hard pauses. Weaning plus a 6 to 8 week lymphatic settle window plus an OB-GYN sign-off is the green zone. Pregnancy is categorically off the table at every trimester. None of that is novel; it’s the consensus across AAP, ACOG, LactMed, InfantRisk, and major lactation-medicine literature. What changes between clinics is whether they respect that consensus or work around it.
At our supervised laser tattoo removal program at Perfect B in Doral the protocol is built into the consult itself, not bolted on afterward. We’ll map your real timeline against your wean date, your OB-GYN sign-off, your Fitzpatrick phototype, and your tattoo’s ink load before any device touches your skin. If today isn’t the right session date for your laser tattoo removal pregnancy or postpartum question, you leave with the right session date in writing, and a one-page summary you can take to your obstetric or pediatric provider before we move forward.
- 📍 Visit us at Perfect B | 3905 NW 107th Ave, Suite 104, Doral FL 33178
- 📞 Call or message us at (786) 502-2260
- 💳 Buy Now Pay Later available: Cherry, Klarna, Afterpay, CareCredit


